Download
1 / 46
780 likes | 2.97k Views
Cardiogenic shock. Greater Twin Cities Area Chapter of AACN Fall Symposium. Kasia Hryniewicz, M.D. November 8, 2013. Minneapolis Heart Institute, Abbott Northwestern Hospital, Minneapolis, MN. Definition.

E N D
Cardiogenic shock Greater Twin Cities Area Chapter of AACN Fall Symposium Kasia Hryniewicz, M.D. November 8, 2013 Minneapolis Heart Institute, Abbott Northwestern Hospital, Minneapolis, MN
Definition • Cardiogenic shock (CS) is a clinical condition of inadequate tissue perfusion due to cardiac dysfunction.
Definition cont • persistent hypotension (systolic blood pressure <80 to 90 mmHg or mean arterial pressure 30 mmHg lower than baseline) • severe reduction in cardiac index (<1.8 L/ min per m2 without support or <2.0 to 2.2 L/ min per m2 with support) • adequate or elevated filling pressures
Etiology Cardiogenic shock Chronic Acute • End stage cardiomyopathy, inotrope dependent
Etiology – Acute CS • Acute myocardial infarction • Large infarct, reinfarction • Mechanical complications MR, VSD, free wall rupture • Right ventricular infarction 2. Non-infarct related - acute myocarditis - acute MR – chordal rupture/endcarditis - acute AI – dissection, endocarditis - stress induced cardiomyopathy - myocardial contusion
Incidence- SHOCK registry • 1190 pts- overall incidence – 5% • The majority of patients have a STEMI, but CS occurs in 2.5% (NSTEMI)
Shock - pathophysiology Hochman J:Circulation 107:2998, 2003
Risk factors • Older age • Anterior MI • Hypertension • diabetes mellitus • multivessel coronary artery disease • Prior MI or diagnosis of heart failure • STEMI • Left bundle branch block on the electrocardiogram (ECG)
Risk factors continue • In the GUSTO-I and GUSTO-III trials of fibrinolytic therapy in acute STEMI • Age • systolic blood pressure • heart rate • Killip class were major predictors of CS accounting for over 95 percent of the predictive information.
Symptoms • severe systemic hypotension • signs of systemic hypoperfusion (eg, cool extremities, oliguria, and/or alteration in mental status) • respiratory distress due to pulmonary congestion. Not all patients present with this syndrome. In particular, most patients develop shock after presentation.
Onset Based on GUSTO trials • Shock was present on admission in 0.8 % at hospital presentation and an additional 5.3 % developed shock after admission, either as a sudden event or as a gradual fall in blood pressure. • Approximately 50 percent of patients who developed shock afteradmission did so within the first 24 hours after the infarct. In SHOCK trial: the median time from MI to onset of cardiogenic shock was 5.5 hours and 75 % of patients developed shock within 24 hours.
Onset cont • Shock developed significantly later among patients with a NSTEMI (median 76 to 94 hours versus 9.6 hours for those with STEMI).
Pre-shock COMMIT trial randomization to early beta blockade was associated with a 30% higher occurrence of CS in patients: • > 70 years of age • SBP < 120 mm Hg • HR >110 beats per minute • Killip Class > 1 Commit trial.
Diagnosis is key! • H&P • ECG • Echo (TTE/TEE) • S-G catheter • Coronary angiogram
Shock trial • Inclusion criterion: shock due to LV failure complicating myocardial infarction • 302 ptsrandomly assigned to emergency revascularization (n=152) or initial medical stabilization (n=150).
Shock trial • IABP was performed in 86 percent of the patients in both groups. • The primary end point mortality from all causes at 30 days. • Secondary end pointsix-month survival
Shock trial results • No difference in mortality at 30 days (46.7% vs 56%, p=0.11) • - Significant decrease in all cause mortality at 6 months (50.3% vs. 63.1% p=0.027).
Shock trial – what have we learned? 1. Average LV ejection fraction (EF) is only moderately severely depressed (30%), with a wide range of EFs and LV sizes noted. 2. SVR on vasopressors is not elevated 3. A clinically evident systemic inflammatory response syndrome is often present in patients with CS. 4. Most survivors have NYHA class I status.
Predictors of outcome • Coronary anatomy-Higher mortality in pts with a LM SVG lesion than in those with LCX, LAD or RCA (79 and 70 %vs37and 42%). RCA culprit lesions were associated with the best prognosis • Echocardiographic predictors- (LVEF) and severity of mitral regurgitation (MR). LVEF <28 percentsurvival at one year was 24% vs 56% Moderate or severe MR survival at one year was 31 % vs 58% However, there was benefit of early revascularization at all levels of LVEF and MR grade. • Symptom onset to reperfusion time- mortality only 6.2 percent in patients reperfused within two hours of symptom onset
Methods • Randomized, prospective, open-label, multicenter trial • 600 patients with CS complicating acute myocardial infarction, randomly assigned to - IABP, (301 pts) or - no IABP (299 pts) plus early revascularization • The primary end point 30-day all-cause mortality. • Safety assessments - major bleeding, peripheral ischemic complications, sepsis, and stroke.
Results • At 30 days – 119 patients in the IABP group (39.7%) and 123 patients in the control group (41.3%) had died (P = 0.69). - At 6 months – no difference in mortality.
Conclusions… • The use of IABP did not significantly reduce 30-day or 6 month mortality in patients with cardiogenic shock complicating acute MI for whom an early revascularization strategy was planned.
Conclusions… The IABP-SHOCK II trial could have affirmed contemporary clinical practice and guidelines,“ "Instead, it revealed surprising results. . . . We must now move forward with the understanding that a cardiovascular condition with 40% mortality at 30 days remains unacceptable
CS-Management • General measures • ventilation support to correct hypoxemia and, in part, acidosis • Optimize intravascular volume • Sodium bicarbonate only for severe metabolic acidosis (arterial pH less than 7.10 to 7.15) • Aspirin • Intravenous heparin • insertion of pulmonary artery catheter
Management cont Pharmacologic support • Vasopressors and inotropes (norepinephrine, vasopressin, dopamine, neosinephrine, dobutamine, milrinone) Mechanical support • IABP??? • Full mechanical support (ECMO?)
Results • 1679 pts,858 dopamine and 821 norepinephrine. • Primary outcome – rate of death at 28 days • Secondary endpoint – number of days without need for organ support and occurrence of adverse events.
Results 1. No difference in primary outcome (52.5% vs 48.5%) 2. Less AE in norepinephrine group (24.1% vs 12.4%, p<0.001) 3. In CS subgroup analysis Dopamine was associated with significantly higher mortality comparing with norepinephrine.
ExtraCorporealMembrane Oxygenation • VV (veno-venous) respiratory failure • VA (veno-arterial) full hemodynamic support for refractory cardiogenic shock • Relatively easy placement • Temporary stabilization, bridge to recovery/permanent VAD • Requires anticoagulation
ECMO at ANWH • 46 pts between 2012-2013 • Percutanously placed in the cath lab • Survival to discharge 70% • Major complications – bleeding • Patients managed by HF cardiologists/RNs/perfusionists in CT ICU
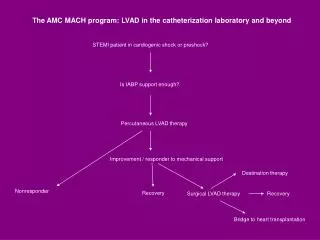
Approach to a pt with CS H&P, ECG, echo (TEE) IABP?/MCS (ECMO)? Acute MI Mechanical complications Severely depressed EF, STE Cath lab Surgery Revascularization PCI MCS (ECMO?)