Download
1 / 23
230 likes | 363 Views
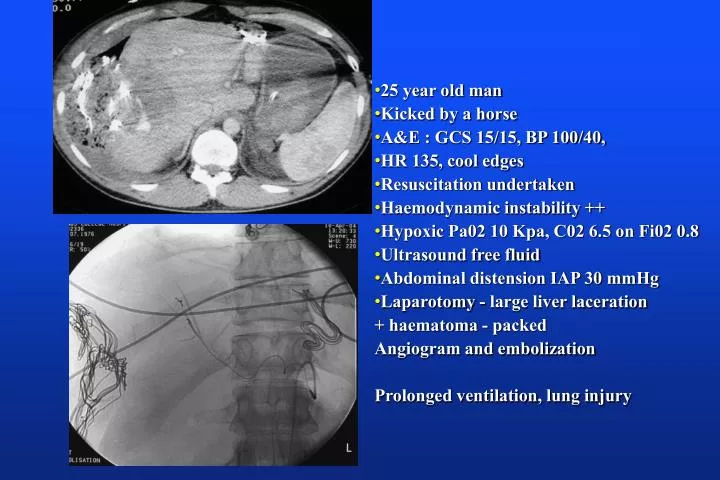
25 year old man Kicked by a horse A&E : GCS 15/15, BP 100/40, HR 135, cool edges Resuscitation undertaken Haemodynamic instability ++ Hypoxic Pa02 10 Kpa, C02 6.5 on Fi02 0.8 Ultrasound free fluid Abdominal distension IAP 30 mmHg Laparotomy - large liver laceration

E N D
25 year old man • Kicked by a horse • A&E : GCS 15/15, BP 100/40, • HR 135, cool edges • Resuscitation undertaken • Haemodynamic instability ++ • Hypoxic Pa02 10 Kpa, C02 6.5 on Fi02 0.8 • Ultrasound free fluid • Abdominal distension IAP 30 mmHg • Laparotomy - large liver laceration + haematoma - packed Angiogram and embolization Prolonged ventilation, lung injury
Buts lets not forget the Medical patients …. Ascites Endoscopy IAP increases Hypoxia ++
Mechanisms • Diaphragms move cranially • Decreased compliance of respiratory system : static and dynamic (Sharp 1986) • Decreased lung volumes, FRC and FRC, expired reserve volume • Pleural pressure increases : predominately in cuadal and dependant regions: airway closure and atelectasis • V/Q mismatch • Decreased vital capacity, increased work of breathing -------resulting in activation of respiratory muscles and increased electromechanical efficacy • In ascites : Decrease VTV, increase RR Abelman 1954, Dempsey 1966 • Increase in PD fluid volume : decrease lung volume, increase diaphragm length, increase maximal insp and transdiaphragmatic pressure Prezant 1990
Gilroy Am J Physiol 1985 • Gastric distension in healthy volunteers : 1 L saline • Changes in lung volume (33%) • Volume rib cage (40%) • Volume abdomen (26%)
Obese and normal subjects undergoing elective abdominal surgery • Static respiratory and lung compliance markedly decreased in the obese population • Laparotomy resulted in improved lung compliance and decreased respiratory resistance Auler Anesth Analg 2002 94(3):741 • Open cholecystectomy vs abdominal wall lift vs C02 insufflation • Insufflation : increased left and right sided pressures • Decreased CI, deranged respiratory mechanics, PIP, lower respiratory compliance. No change in dead space to TV ratio • Galizia Surg Endosc 2001 15(5):477, Nguyen Surg Endosc 2004 18(1):64
Laparoscopic surgeryAnderson Acta anaesth Scand 2003 ;47:838 • Pneumoperitoneum vs abdominal wall lift :lap choly • Supine, head up and head up 30 degrees • No changes in Vtv, Fi02 during study protocol • P max in insufflation group 25 ±4 vs 17 ±5 cmH20. Similar changes seen with head tilting • Significant increase in intraoesophageal pressure
D’Angelo Resp Physiol and Neurobiol 2002 130:293 • Examine the effect of abdominal distension on diaphragm and rib cage muscle function in supine and head up (600) with and without vagaotomy……rabbits…. Monitored / abdominal balloons inserted 0.69 + 0.96 L • Initially spontaneous breathing and then paralysed to obtain pressure volume curves • Baseline : tilting did not change VC but FRC was increased • Increased IAP shifted curves to right and down for the respiratory system and chest wall • VC (4 -33%) and FRC (20 +53%) supine • VC ( 6 - 39%) and FRC (25-49%) head up • Lung effects small
Deflation V-P curves for respiratory system, chest wall and lungsD’Angelo Resp Physiol and Neurobiol 2002 130:293 RS lung CW
D’Angelo Resp Physiol and Neurobiol 2002 130:293 • Acute AD in spontaneously breathing rabbits • changed patterns of activation and electromechanical efficiency of the inspiratory muscles • Tonic inspiratory muscle activity, inspiratory prolongation and improved efficiency of parasternal muscles • modifed the elastic properties of the respiratory system • Changes in the electromechanical efficiency of the diaphragm depended upon posture and degree of AD • Upright posture + intermediate AD : increased efficiency which along with parasternals resulted in an increase in TV • Larger levels of AD, and all levels in the supine posture result in decreased electromechanical efficiency of the diaphragm with a fall in TV
Inflammatory response • Rat study increased IAP 20 mmHg for 60 and 90 minutes - held for 60 minutes then decompress and sample after 30 minutes • Increased IL-1 seen at 60 minutes IAP • Increased IL-6 and TNF at 30 mins decompression • Increased lung neutrophils, histology pulmonary infiltrates, atelactasis and oedema • Rezende-Neto J Trauma 2002 53(6):1121 • IAP 20 for 60 mins then normal 60 mins : increased monodialdehde and myeloperoxidase levels in lung and kidney. • Decreased GSH on reperfusion • Kacmaz Peptides 2003 24 (9) : 1381 • Hsu J Trauma 2004 57(3):569
IAP and inflammation and ALIQuintel Am J Resp Crit Care Med 2004 169:534 Examined CT/respiratory and haemodynamic variables in healthy and oleic acid injured lungs at IAP of 0 and 20 cmH20. Pressure volume curves undertaken Ventilated at 12 ml/Kg, PEEP5 rate 12-14 Fi02 1.0 • Healthy lung + IAP 20 ----- decreased gas content, tissue content stable, increased non aerated tissue • Oleic acid + IAP 0 ----- decreased gas content and increased tissue mass (30±24% of original) : base regions • Oleic acid IAP 20 ------marked decrease in gas content and increase in tissue mass (103±37%) : homogenous • No change in tissue mass over time in control animal treated with oleic acid but no IAP elevation
Mechanics In healthy tissue although gastric pressure rose I/oesoph was unchanged At 100 ml inflation increase in elastance due to chest wall whilst at 500 ml there was a lung component. Oleic tissue : Gastric and oesophageal pressures increased as did the elastance of the system mainly due to lung component
Gas -grey bars tissue solid bars Left bar 0 IAP Right bar 20 IAP Tissue content was higher at IAP 20 cmH20 than 0 Gas content was lower at 20 than 0 cmH20 IAP Total lung tissue similar at 0 and 20 At 20 cm H20 IAP total gas volume decreased at each interval by approx 50%
Increased ITBVI/PBV would not account for the level of increase seen in tissue volume • These data suggest that increase tissue mass is lung oedema • Increased production of oedema in association with increased IAP ? Related to PAOP pressure changes • Impaired clearance of oedema • Lymphatics, pulmonary capillaries and pleural capillaries draining via thoracic veins • Intra-oesophageal pressure 3 X normal • Intrathoracic pressure elevation impedes lymph flow • If these data can be extrapolated to man increased IAP may not only decrease oxgenation by reducing gas content but also by increasing lung leak
So what about proning people ? Many of those with ARDS also have increased IAP if measured
Position, ALI and IAP Hering et al Anesth Analg 2001 92(5):1226 16 patients with ALI underwent prone positioning IAP 12 ± 4 to 14 ± 5 mmHg Pa02/Fi02 ratio 220±96 to 267±82 mmHg p<0.05 MAP 77±10 to 82 ± 11 mmHg p<0.01 RVRI 1172 ± 6554 to 15078 ± 10594 GFR, filtration fraction, urine volume, urinary Na excretion, free water clearance unchanged Abdominal release in the prone position does not improve Oxygenation in an experimental model of ALI Colmenero-Ruiz Int Care Med 2000
Proned with abdominal distensionMure Am J Resp Crit Care Med 1998;157:1785 • Pulmonary gas exchange supine and prone ± AD in pigs • Ventilated Fi02 0.4, RR 27, TV 13-15 ml/kg, normocapnia • Prone normal abdomen: Pa02 increased by 16 ± 21 mmHg **, no other haemodynamic or gas exchange variables changed • AD resulted in : compliance decreased, PIP and plateau pressures increased as did VA/Q heterogeneity, FRC decreased • Prone with AD • Increased Pa02 26±18**, decreased A-aP02, decreased heterogeneity** • Plateau pressures decreased, no changes in compliance • Decreased V/Q heterogeneity • Gastric pressure fell 24±8 to 18=9 cmH20 • Normally increased Pleural pressure leading to atelectasis at FRC when prone pleural pressure becomes more negative in the dependant areas than when supine : more open airways
Intra-abdominal hypertension and lungs • Intrathoracic pressures, intracardiac pressures, intracranial pressures may all be affected • Decreases LV, respiratory and chest wall compliance • Assessment of preload requires dynamic and volumetric parameters to prevent tissue hypoperfusion : SVV , SPV, ITBVI, GEDVI, echo • Inflammatory component in lungs (? Isch/reperfusion) • Hypoxia may or may not reflect increased lung water • Need to measure it ? • Set PEEP to counteract IAP • Lung protective strategies aim for delta P plateau (plateau pressure - IAP) • Consider position and diaphragmatic function in a dynamic manner • Try to do no harm
D’Angelo et al At all volumes of AD changes in end Expiratory lung volumes were mirrored in Transverse diameter of ribs Larger pre vagotomy and larger when supine At low AD no changes As AD increased change in end expiratory lung volumes and was larger in the head up position and post vagotomy Changes in end exp volumes were accompanied by increase in inspired Time and decrease in expired : lost post vagotomy
Effects if IAH on respiratory function • Data has been obtained from • Normal volunteers • Studies in obese and ascitic individuals • Laparoscopic surgery • Animal studies • Spontaneous breathing • Effect of position