Download
1 / 46
• 460 likes • 478 Views
Explore case #72 of a 57-year-old patient with challenging coronary artery disease, failed procedures, and ongoing symptoms. Learn about retrograde techniques, success patterns, updates in appropriate revascularization practices, and procedural outcomes.

E N D
Complex Coronary Cases Supported by: Abbott Vascular Inc Boston Scientific Corp Terumo Vascular Corp Vascular Solutions Inc Cardiovascular Science Inc AstraZeneca Pharmaceuticals The Medicines Company Trireme Medical
Disclosures Samin K. Sharma, MBBS, FACC Speaker’s Bureau – Boston Scientific Corporation, Abbott Vascular Inc, AngioScore, ABIOMED, CSI, Trireme Medical Annapoorna S. Kini, MBBS, FACC Nothing to disclose Sameer Mehta, MBBS, FACC Consulting Fees – The Medicines Company
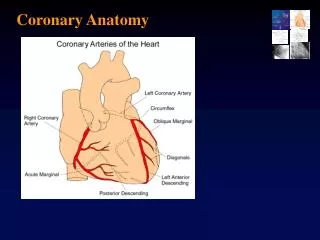
June 16th 2015 Case #72: CW, 57 yrs M Presentation: Patient presented with new onset CCS Class IV angina. A cardiac cath on April 6th 2015 revealed 2 V CAD (CTO of RCA and subtotal occlusion of LCx-LPL branch), LVEF 60% and SYNTAX score 24. Pt underwent successful intervention of LCx-LPL branch with DES (2and failed attempt at antegrade recanalization of CTO RCA. No complications and discharged next day. Pt continued to have Class II angina and a stress MPI revealed moderate inferior wall ischemia. Prior History: Hypertension, Hyperlipidemia Medications: All once daily dosage Lisinopril 10mg, Rosuvastatin 20mg, ASA 81mg, Prasugrel 5mg, Nebivolol 5mg, ISMN 60mg
Case# 72: cont… Cardiac Cath 4/6/2015: Right Dominance II V CAD with LVEF 60% LM: No obstruction LAD: 30% prox LAD lesion LCx: mild diffuse disease, 99% LPL1 RCA: 100% prox occlusion, distal vessel fills via LAD-S2 Pt underwent PCI of LCx-LPL with Xience Alpine DES (2.5/15mm) with excellent results, but failed RCA CTO recanalization SYNTAX Score was : 24 Plan Today: PCI of CTO RCA via retrograde approach due to failed antegrade approach
Issues Involving The Case • Current status of Retrograde CTO Recanalization • Update in Appropriate Use Criteria (AUC) for PCI
Issues Involving The Case • Current status of Retrograde CTO Recanalization • Update in Appropriate Use Criteria (AUC) for PCI
Retrograde Wire Technique for Chronic Total Occlusion Recanalization Four Patterns of Success in Retrograde CTO Recanalization Sumitsuji et al. J Am Coll Cardiol Intv 2011;4:941.
Summary of Published Retrograde CTO PCI Series Karmpaliotis et al., JACC Cardio Interv 2012;5:1273
ERCTO Registry: Numbers of Procedures and Rate of Procedural Success Antegrade, Retrograde, and Total PCI Volumes from 2008 to 2012 Procedural Success Rates per Year – Significant Increase Galassi et al., J Am Coll Cardiol 2015;65:2388
ERCTO Registry: Procedural Characteristics According to Procedural Success (2008 – 2012) Galassi et al., J Am Coll Cardiol 2015;65:2388
ERCTO Registry: Procedural Success According to J-CTO Score and Operator Experience Galassi et al., J Am Coll Cardiol 2015;65:2388
ERCTO Registry: Univariate and Multivariate Logistic Regression Modelling, Procedural Failure Galassi et al., J Am Coll Cardiol 2015;65:2388
ERCTO Registry: Procedural Complications and In-Hospital Outcomes in Retrograde Lesions (2008 – 2012) Galassi et al., J Am Coll Cardiol 2015;65:2388
ERCTO Registry: Clinical Outcome at 3 years According to Procedural Success Overall Successful Unsuccessful p=<0.001 p=<0.001 % p=0.001 p=0.014 p=0.120 MACCE Cardiac death MI Stroke Revasc Galassi et al., J Am Coll Cardiol 2015;65:2388
ERCTO Registry: Sustained Symptomatic Benefit Galassi et al., J Am Coll Cardiol 2015;65:2388
Retrograde CTO PCI: 5 Steps Retrograde PCI for recanalization of CTOs has gained acceptance as a necessary technique to improve success The procedure involves five key steps: • Wiring of the collateral from the donor artery into the distal bed of the recipient artery, usually with the use of hydrophilic jacketed guidewires • Delivery of over-the-wire microcatheters especially Corsair channel dilator to allow an exchange for a CTO-specific guidewire • Crossing the total occlusion with the CTO guidewire and dilating the CTO with the retrograde small balloon (1.25-1.5/8-10mm size) • Placing an antegrade guidewire into the distal bed through the recanalized CTO. Rarely exteriorization of the long retrograde guidewire (Viper wire 360cm) is needed to advance antegrade monorail or over-the-wire small balloon 5. Stenting the lesion over the antegrade guidewire
Retrograde Wire Technique for CTO Recanalization • When to do Retrograde technique? • Minimum 200 CTO cases via antegrade technique • Dedicated setup, equipment and ability to handle compl. • Usually after failed antegrade (once or twice) approach • Ostial stump occlusion (RCA, LAD, LCx)
Issues Involving The Case • Current status of Retrograde CTO Recanalization • Update in Appropriate Use Criteria (AUC) for PCI
ACCF/SCAI/STS/AATS/AHA/ASNC 2012Appropriateness Criteria for Coronary Revascularization ACCF/SCAI/STS/AATS/AHA/ASNC 2009Appropriateness Criteria for Coronary Revascularization Patel et al. JACC 2009;53:530-553 Patel et al. JACC 2012;59:857.
Appropriate Use Criteria (AUC) Elements of Coronary Revascularization Four Essential Elements: • Symptoms: asymptomatic, Class I-II vs. Class III-IV • Non-invasive risk assessment: low, intermediate or high risk • Maximal medical therapy: 2 Drugs- Nitrates, Ca+ blocker, Beta blocker or Ranolazine • Coronary anatomy findings
ACCF/SCAI/STS/AATS/AHA/ASNC 2009Appropriateness Criteria for Coronary Revascularization Noninvasive Risk Stratification High-Risk (greater than 3% annual mortality rate)1. Severe resting left ventricular dysfunction (LVEF less than 35%)2. High-risk treadmill score (score less than or equal to 11)3. Severe exercise left ventricular dysfunction (exercise LVEF less than 35%)4. Stress-induced large perfusion defect (particularly if anterior)5. Stress-induced multiple perfusion defects of moderate size6. Large, fixed perfusion defect with LV dilation or increased lung uptake (thallium-201)7. Stress-induced moderate perfusion defect with LV dilation or increased lung uptake (thallium-201)8. Echocardiographic wall motion abnormality (involving greater than two segments) developing at low dose of dobutamine (less than or equal to 10 mg/kg/min) or at a low heart rate (less than 120 beats/min)9. Stress echocardiographic evidence of extensive ischemiaIntermediate-Risk (1% to 3% annual mortality rate)1. Mild/moderate resting left ventricular dysfunction (LVEF equal to 35% to 49%)2. Intermediate-risk treadmill score (11 less than score less than 5)3. Stress-induced moderate perfusion defect without LV dilation or increased lung intake (thallium-201)4. Limited stress echocardiographic ischemia with a wall motion abnormality only at higher doses of dobutamine involving less than or equal to two segmentsLow-Risk (less than 1% annual mortality rate)1. Low-risk treadmill score (score greater than or equal to 5)2. Normal or small myocardial perfusion defect at rest or with stress3. Normal stress echocardiographic wall motion or no change of limited resting wall motion abnormalities during stress Patel et al. JACC 2009;53:530-553
Appropriateness Ratings by Low-Risk Findings on Noninvasive Imaging Study and Asymptomatic ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Patel et al. JACC 2009;53:530-553
Appropriateness Ratings by Intermediate-Risk Findings on Noninvasive Imaging Study and CCS Class I or II Angina ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Patel et al. JACC 2009;53:530-553
Appropriateness Ratings by High-Risk Findings on Noninvasive Imaging Study and CCS Class III or IV Angina ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Patel et al. JACC 2009;53:530-553
Appropriateness Use Criteria for PCI AUC Criteria from ACC-NCDR Results (n=500,00) 98.6 84.6 ALL ACS PCI (71%) Elective PCI (29%) % 50.4 38.0 11.6 11.2 4.1 1.1 0.3 Inappropriate Appropriate Uncertain Paul Chan. JAMA 2011;306:53.
PCI Volumes by Clinical Indication in Washington State Courage Trial Bradley et al., Circulation 2015, In Press
Calendar Year Trends in PCI Appropriateness: PCI for Acute Indications in Washington State Inappropriate (n=224) Appropriate (n=37,561) p=<0.001 % Bradley et al., Circulation 2015, In Press
Calendar Year Trends in PCI Appropriateness: All PCI for Stable CAD in Washington State Inappropriate Appropriate p=<0.001 % Bradley et al., Circulation 2015, In Press
Calendar Year Trends in PCI Appropriateness By Indication – PCI Mapped to AUC for Stable CAD Inappropriate Appropriate p=<0.001 % Bradley et al., Circulation 2015, In Press
Calendar Year Trends in PCI Appropriateness By Indication for Stable CAD: Washington State Inappropriate Appropriate All-PCI PCI Mapped to AUC p=<0.001 p=<0.001 % % Bradley et al., Circulation 2015, In Press
Temporal Declines in Inappropriate PCIs by Hospital Tertiles Tertile of Middle Temporal Decline Tertile of Smallest Temporal Decline Tertile of Largest Temporal Decline Bradley et al., Circulation 2015, In Press
Calendar Year Trends in PCI Appropriateness: PCI Mapped to AUC in Stable CAD New York State Appropriate Inappropriate % N=14,743 N=14,447 N=10,391
Appropriateness of Revascularization by PCI: NY State vs. MSH for Stable CAD in 2010 NYS MSH NYS MSH NYS MSH % Hannan E et al. JACC 2012;59:1870
MSH Appropriateness of Revascularization by PCI: NYS Data Report Appropriate Category of PCI Inappropriate Category of PCI % %
Referral for Invasive work up of Stable CAD Patient Stable CAD scheduled for Cath CCS Class I or II (> 2 blocks, > 1 flight) Not on MMT Asymptomatic or Low Risk Non Invasive Study CCS Class III IV (<2 blocks, < 1 flight ) and/or High Risk Non Invasive study (EF<35%, large perfusion def) Class III Angina > 2Antianginal Intermediate on non invasive Study (EF, Intermediate perfusion defect) Appropriate Appropriate If not Inappropriate No Yes > Antianginal Appropriate Inappropriate Appropriate Appropriate
Take Home Message:Retrograde CTO recanalization and AUC for PCI • ERCTO registry from Europe revealed that retrograde CTO revascularization is increasing in volume and success with lower procedural complications. Long-term data showed sustained symptomatic benefit of retrograde CTO recanalization. Hence R-CTO should be attempted after failed antegrade approach(s) except in cases of ostial CTOs where could be the first line approach • Widespread implementation of AUC for PCI has resulted in decline in PCI volume for stable CAD along with decline in Inappropriate PCI. PCI done for ACS indications is rarely Inappropriate
Question # 1 ERCTO registry showed that retrograde approaches to CTO recanalization is associated with all except: • Lower CCS angina class at 1-3 yrs • Lower dyspnea at 1-3 yrs • Overall success rate above 90% in recent years • Approx 2-5% procedural complications • Lower revascularization at F/U
Question # 2 Following is the ideal case to attempt retrograde recanalization of CTO as the first line approach: • Mid LAD CTO • Ostial RCA CTO • SVG CTO • Prox LCx CTO • RPDA CTO
Question # 3 In recent years, Inappropriate PCI for stable CAD occurs in following % of cases; A. <5% B. 5-10% C. 10-15% D. 15-20% E. >20%
Question # 1 ERCTO registry showed that retrograde approaches to CTO recanalization is associated with all except: • Lower CCS angina class at 1-3 yrs • Lower dyspnea at 1-3 yrs • Overall success rate above 90% in recent years • Approx 2-5% procedural complications • Lower revascularization at F/U The correct answer is C
Question # 2 Following is the ideal case to attempt retrograde recanalization of CTO as the first line approach: • Mid LAD CTO • Ostial RCA CTO • SVG CTO • Prox LCx CTO • RPDA CTO The correct answer is B
Question # 3 In recent years, Inappropriate PCI for stable CAD occurs in following % of cases; A. <5% B. 5-10% C. 10-15% D. 15-20% E. >20% The correct answer is C