Download
1 / 36
390 likes | 746 Views
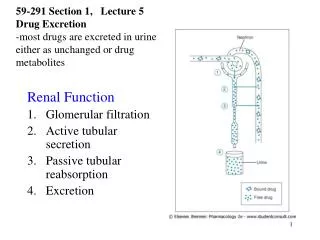
Reabsorption and Secretion. Learning Objectives. Understand how fluid flow from the tubular lumen to the peritubular capillaries. Know how the reabsorption of H 2 O, Cl - , Ca 2+ , Mg 2+ , glucose, and amino acids are coupled to the active transport of Na + .

E N D
Learning Objectives • Understand how fluid flow from the tubular lumen to the peritubular capillaries. • Know how the reabsorption of H2O, Cl-, Ca2+, Mg2+, glucose, and amino acids are coupled to the active transport of Na+. • Understand the function of the proximal tubule, loop of Henle, distal tubule, collecting tubule, and medullary collecting ducts. • Know the renal mechanism for pressure diuresis and natriuesis. • Know how the kidney forms dilute or concentrated urine. • Know how a hyperosmotic renal medulla is established. • Know how antidiuretic hormone, aldosterone and angiotensin II affect renal funciton. • Know how the kidneys help regulate the body’s acid-base balance.
H2O, Cl-, and Urea • Generally, these follow Na+ through electrical forces and osmosis. • Urea is less permeable than H2O and Cl- and thus, is not reabsorbed to the same level.
Secretion in the Proximal Tubule • Bile salts, oxalate, urate and catecholamines are secreted into the proximal tubule. Many of the substances secreted are metabolic end-products. • Many drugs are secreted, including penicillin. • Para-aminohippuric acid (PAH) is rapidly secreted through the same transporter used to secrete penicillin. PAH is a derivative of para-aminobenzoic acid (PABA) – used by bacteria to make folic acid. • In WW II, PAH was administered with penicilin to decrease Penicillin’s secretion. Probenecid was also used for this purpose.
Flow of Fluid into the Peritubular Capillaries Top panal: Normal Bottom panal: Increased peritubular capillary hydrostatic pressure or decreasing osmotic pressure.
Forming a Dilute Urine Key to this antidiuretic hormone (ADH) or vasopressin, which increases the permeability of the distal tubules and collecting ducts to H2O. When there is excess H2O in the body, ADH levels are low so that little H2O is reabsorbed in the distal tubule and collecting ducts. However, Na+, K+, and Cl- are reabsorbed.
Forming a Concentrated Urine • H2O is reabsorbed in the distal tubule and collecting ducts. • 2 Keys: - High level of ADH, to increase H2O reabsorption in the distal tubules and collecting ducts. - A high osmolarity of the medullary interstitial fluid. • What process makes the medullary interstitial fluid hyperosmotic?
Countercurrent Mechanism Actually, the Na+ will make the medullary interstitial fluid ~ 600 mOsm/L Urea, in the presence of ADH, contributes to achieve 1,200 mOsm/L.
Urea When there is a H2O deficit and ADH is high, urea becomes concentrated in the distal tubule and cortical collecting tubule when H2O is reabsorbed. This high [urea] reaches the medullary collecting duct. There, ADH increases permeability to urea and activates urea transporters. Thus, urea diffuses out into the interstitial fluid and increases the osmolarity. The high osmolarity of the medullary interstitium increase H2O absorption when H2O permeability is high (ADH). This creates a concentrated urine.
Hormones Controlling Renal Function • ADH or Vasopressin - Increases H2O permeability of the distal tubul, cortical collecting tubule, and medullary collecting tubule. Also, - Increases the permeability of urea in the medullary collecting tubule. • Aldosterone – stimulates the Na+-K+-ATPase in the cortical collecting tubule. • Angiotensin II - Stimulates aldosterone secretion. - Constricts efferent arterioles. - Stimulates Na+-K+-ATPase in the proximal tubule, loops of Henle, distal tubules and collecting tubules.
Regulation of pH • 3 Primary systems for regulating the pH of the body: 1. Acid-base buffers of the body fluids. 2. Removal of CO2 via respiration. 3. Renal excretion of acid or alkaline urine. • Today, we will briefly cover the bicarbonate buffer and renal mechanisms.
Renal Control of Acid-Base Balance The balance is achieved by regulating the secretion of H+. Bicarbonate must react with H+ before it can be reabsorbed. If H+ is low, the kidneys do not reabsorb as much bicarbonate, increasing the amount of bicarbonate excreted. If H+ is high, the kidneys reabsorb nearly all the bicarbonate. The excess H+ in the tubular lumen combines with phosphate and ammonia and is excreted as salts.