Download
1 / 96
960 likes | 994 Views
Learn about the impact of acid-base properties on drug behavior, using pKa and Henderson-Hasselbalch equation. Explore examples of acids, bases, and their ionization degrees, and understand the significance in pharmaceutical chemistry.

E N D
Lecture 3Organic Pharmaceutical ChemistryY3Acid-Base properties of DrugsQSAR
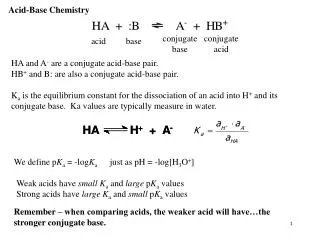
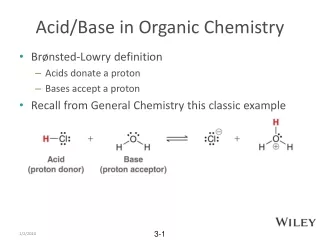
Acid-Base Properties of Drugs Most drugs used today are classified as acids or bases. Acid-base properties of a drug can greatly influence its biodistribution and partitioning characteristics. The definition of Bronsted - Lowry is widely used in pharmacy. An acid is a proton donor and a base is defined as a proton acceptor. Acid + base ═ Conjugate acid + Conjugate base
Acid Strength determines how one predicts in which direction an acid-base reaction lies and to what extent the reaction goes to completion. The pKa contains the information to answer these questions. Hinderson- Hasselbalch equation can be used to calculate the pH of weak acids, weak bases and buffers consisting of weak acids and their conjugate bases.
Sometimes pKb is used for bases. The two are related by the equation pKa = pKb-14. It is important to recognise that the pKa of the base is in reality the pKa of the conjugate acid (acids are proton donors HA, or protonated form, BH+) of the base. The pKas for ephedrine and ammonia are 9.6 and 9.3 respectively. In reality this is the pKa of the protonated form, such as ephedrine hydrochloride and ammonium chloride respectively.
Remember that pKas indicate the extent to which the acid reacts with water to form conjugate acid and conjugate base. The equilibrium for a strong acid (low pKa) in water lies to the right favoring the formation of products (conjugate acid and conjugate base). This means that there essentially is no unreacted HCl left in the aqueous solution of hydrochloric acid. Equilibrium for a weak acid (high pKa) lies to the left.
At the other extreme is ephedrine HCl with a pKa of 9.6. Here the denominator representing the concentration of ephedrine HCl greatly predominate against the products, which in this example is ephedrine and H3O+. In other words the protonated form of ephedrine is very proton donor and free ephedrine is an excellent proton acceptor. A general rule for determining whether a chemical is a strong or weak acid or base, from pKa values, is
pKa less than 2: Strong acid; conjugate base has no meaningful basic properties in water pKa 4-6: weak acid, weak conjugate base pKa 8-10: very weak acid, conjugate base getting stronger pKa greater than 12: essentially no acidic properties in water; strong conjugate base.
The values of pKa and pKb quoted in the literature tell absolutely nothing about whether the drug in question is an acid or base. These values give information about the strength of acids or bases; they tell the pH at which 50% of the drug is ionised, but they do not tell whether a drug behaves as an acid or base in solution. Amines, for example are basic and have pKa values of approximately 9, while phenols are acidic and typically have pKa values of around 10.
The only way to know whether a drug is acidic or basic is to learn the functional groups that confer acidity or basicity on a molecule. Carboxylic acids The carboxyl group is the most commonly occurring functional group on drug molecules.. Q1: The pKas of acetic acid and ethanol are 4.7 and 16 respectively. Comment on such a difference.
Q2: A number of commonly used drugs are carboxylic acid derivatives. These include aspirin (pKa 3.5), the anticancer compound methotrexate (pKa 3.8, 4.8 and 5.6) and the diuretic furosemide (pKa 3.9). The structures of these compounds are shown below. Explain the difference in pKas of these compounds and comment on the degree of ionisation of these drugs at the pH of human blood. .
Phenols Phenols are weak acids that liberate protons to give the resonance stabilised the phenoxide anion. They have pKa values of approximately 10. A number of common drugs contain the phenol functional group. These include paracetamol, morphine and levothyroxine of pKas 9.5, 9.9 and 10 respectively. They will ionise to approximately 1% at the pH of blood
Warfarin is an anticoagulant drug that inhibits the clotting action of blood through an action on vitamin K-derived clotting factors. It has a pKa of 5.0 and in the free acid form is not soluble in water and is therefore admistered as the sodium salt. Warfarin exhibits keto-enoltautomerisation. Although the enol tautomer is present in small extent, it can be used to explain the acidic properties of the drug.
Amines Not all compounds containing nitrogen atom(s) are basic. Amides are neutral and quite few drugs containing nitrogen atoms are actually acidic. Compounds are basic only if the lone pair of electrons on the nitrogen is available for reaction with protons.
Phenylbutazone is a NASID drug that exerts an anti-inflammatory action through inhibition of the enzyme cyclooxygenase. It is a weak acid with pKa of 4.4. Indometacin is another NASID with a similar mode of action to that of phenylbutazone with pKa of 4.5.
Barbiturates are cyclic imides used as hypnotics. They are all derivatives of barbituric acid which is not pharmacologically active. They behave as weak acids, diprotic. The delocalisation is similar to that of warfarin and the pKas range from 7-8 for the first ionisation and 11-12 for the second ionisation. The drugs are usually administered as sodium salts to increase water solubility.
The sulfur analogue of pentobarbital, the thiopental, is widely used in operating theatres for the induction of general anesthesia. When thiopental are adminisred intravenously to a vein in the back of the hand it will induce unconsciousness within a second and will last for few minutes, which is sufficient time for preparation of a patient to commence general anesthesia.
Phenytoin is an anticonvulsant widely used in the treatment of epilepsy. Its properties resemble those of barbiturates, pKa of 8.3 and like the barbiturates display tautomerism of imine-imide type, the imide is predominant. Sulphonamides are antibacterial compounds, contain the sulfonamide group SO2NH. They are all weakly acidic pKa approximately 5-8. They are usually administered in the form of sodium salts to increase water solubility.
Basic drugs They are usually administered as their water soluble salts ( generally the hydrochloride). Care must be taken not to coadminister anything that will raise the pH of the hydrochloride salt solution in case precipitation of the less water-soluble free base occurs. Basicity of heterocyclic compounds Piperidines - pKa 8-9 Pyrroles, pKa -ve - zero Pyridines, pKa4-5
Examples of calculations requiring the pKa Ex: What is the ratio of ephedrine to ephedrine HCl (pKa 9.6) in the intestinal tract at pH 8.0?
The number whose log is - 1.6 is 0.025, meaning that there are 25 parts ephedrine for every 1,000 parts ephedrine HCl in the intestinal tract whose environment is pH 8.0. What is the pH of a buffer containing 0.1-M acetic acid (pKa 4.8) and 0.08-M sodium acetate? What is the pH of a 0.1-M acetic acid solution? Use the following equation for calculating the pH of a solution containing either an HA or BH+ acid.
What is the pH of a 0.08-M sodium acetate solution? Remember, even though this is the conjugate base of acetic acid, the pKa is still used. The pKw term in the following equation corrects for the fact that a proton acceptor (acetate anion) is present in the solution. The equation for calculating the pH of a solution containing either an A- or B base is
What is the pH of an ammonium acetate solution? The pKa of the ammonium (NH4+) cation is 9.3. Always bear in mind that the pKa refers to the ability of the proton donor form to release the proton into water to form H3O+. Since this is the salt of a weak acid (NH4+) and the conjugate base of a weak acid (acetate anion), the following equation is used. Note that molar concentration is not a variable in this calculation.
What is the percentage ionization of ephedrine HCl (pKa 9.6) in an intestinal tract buffered at pH 8.0 (see example 1)? Use Equation 2.4 because this is a BH+ acid. Only 2.4% of ephedrine is present as the un-ionized conjugate base. What is the percentage ionization of indomethacin (pKa 4.5) in an intestinal tract buffered at pH 8.0? Use Equation 2.3 because this is an HA acid.
A general rule for determining whether a chemical is strong or weak acid or base For all practical purposes, indomethacin is present only as the anionic conjugate base in that region of the intestine buffered at pH 8.0. pKa<2: strong acid; conjugate base has no meaningful basic properties in water pKa 4 to 6: weak acid; weak conjugate base pKa 8 to 10: very weak acid; conjugate base getting stronger pKa >12: essentially no acidic properties in water; strong conjugate base
This delineation is only approximate. Other properties also become important when considering cautions in handling acids and bases. Phenol has a pKa of 9.9, slightly less than that of ephedrine HCl. Why phenol is considered corrosive to the skin, whereas ephedrine HCl or free ephedrine is considered innocuous when applied to the skin? Phenol has the ability to partition through the normally protective lipid layers of the skin. Because of this property, this extremely weak acid has carried the name carbolic acid. Thus, the pKa simply tells a person the acid properties of the protonated form of the chemical. It does not represent anything else concerning other potential toxicities.
Percent Ionization Using the drug's pKa, the formulation or compounding pharmacist can adjust the pH to ensure maximum water solubility (ionic form of the drug) or maximum solubility in nonpolar media (un-ionic form). This is where understanding the drug's acid-base chemistry becomes important:
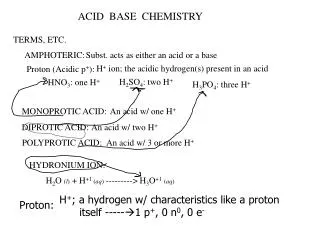
Acids can be divided into two types, HA and BH+, on the basis of the ionic form of the acid (or conjugate base). HA acids go from un-ionized acids to ionized conjugate bases. In contrast, BH+ acids go from ionized (polar) acids to un-ionized (nonpolar) conjugate bases. In general, pharmaceutically important HA acids include the inorganic acids (e.g., HCl, H2SO4), enols (e.g., barbiturates, hydantoins), carboxylic acids (e.g., low-molecular-weight organic acids, arylacetic acids, N-aryl anthranilic acids, salicylic acids), and amides and imides (e.g., sulfonamides and saccharin, respectively). The
The chemistry is simpler for the pharmaceutically important BH+ acids: They are all protonated amines. A polyfunctional drug can have several pKa's (e.g., amoxicillin). The latter's ionic state is based on amoxicillin's ionic state at physiological pH 7.4. The percent ionization of a drug is calculated by using Equation 2.3 for HA acids and Equation 2.4 for BH+ acids.
Increasing the hydrogen ion concentration (decreasing the pH) will shift the equilibrium to the left, thereby increasing the concentration of the acid and decreasing the concentration of conjugate base. In the case of indomethacin, a decrease of 1 pH unit below the pKa will increase the concentration of un-ionized (protonated) indomethacin to 9.1%. Similarly, a decrease of 2 pH units results in only 0.99% of the indomethacin being present in the ionized conjugate base form.
The opposite is seen for the BH+ acids. The percentage of ephedrine present as the ionized (protonated) acid is 90.9% at 1 pH unit below the pKa and is 99.0% at 2 pH units below the pKa. With this knowledge in mind, return to the drawing of amoxicillin. At physiological pH, the carboxylic acid (HA acid; pKa1 2.4) will be in the ionized carboxylate form, the primary amine (BH+ acid; pKa2 7.4) will be 50% protonated and 50% in the free amine form, and the phenol (HA acid; pKa3 9.6) will be in the un-ionized protonated form.
Knowledge of percent ionization makes it easier to explain and predict why the use of some preparations can cause problems and discomfort as a result of pH extremes. Phenytoin (HA acid; pKa 8.3) injection must be adjusted to pH 12 with sodium hydroxide to ensure complete ionization and maximize water solubility. In theory, a pH of 10.3 will result in 99.0% of the drug being an anionic water-soluble conjugate base. To lower the concentration of phenytoin in the insoluble acid form even further and maintain excess alkalinity, the pH is raised to 12 to obtain 99.98% of the drug in the ionized form.
Even then, a cosolvent system of 40% propylene glycol, 10% ethyl alcohol, and 50% water for injection is used to ensure complete solution. This highly alkaline solution is irritating to the patient and generally cannot be administered as an admixture with other intravenous fluids that are buffered more closely at physiological pH 7.4. This decrease in pH would result in the parent un-ionized phenytoin precipitating out of solution.
Adjustments in pH to maintain water solubility can sometimes lead to chemical stability problems. An example is indomethacin (HA acid; pKa 4.5), which is unstable in alkaline media. Therefore, the preferred oral liquid dosage form is a suspension buffered at pH 4 to 5. Because this is near the drug's pKa, only 50% will be in the water-soluble form. There is a medical indication requiring intravenous administration of indomethacin to premature infants. The intravenous dosage form is the lyophilized (freeze-dried) sodium salt, which is reconstituted just prior to use.
Ionization – pH Profiles The plot of percent ionisation versus pH for an HA acid (indomethacin, pKa 4.5) and an HB+(ephedrine, pKa 9.6) illustrates how the degree of ionisation can be shifted significantly with small changes in pH. Similar sketches can made for any acid. When the pH = pKa the compounds are 50% ionised. An increase by 1 pH unit from the pKa of indomethacin results in 90.9% but decrease the ionisation of ephedrine HCl to 9.1%.
This highly alkaline solution is irritating to the patient and generally cannot be administered as an admixture with other intravenous fluids that are buffered more closely at physiological pH 7.4. This decrease in pH would result in the parent unionised phenytoin precipitating out of solution. The acidic eye drops tropicamidepKa of 5.2 can sting, pH of 4 to obtain more than 90% ionisation. Local anesthetic eye drops are used to minimise the patient's discomfort.
Chemical stability of a drug can sometimes be affected by pH adjustments. An example is iodomethacin of pKa 4.5 which is unstable in alkaline media. IV dosage of the lophylised ( freeze - dried ) sodium salt, which is reconstituted just prior to use. Drugs in an ionised form will tend to distribute by the blood throughout the body more rapidly than unionised, nonpolar, molecules.
In general drugs pass through the nonpolar membranes of the capillary walls, cell membranes and the blood-brain barrier in the unionised (non-polar) form. For HA acids, it is the parent acid that will readily cross these membranes. The situation is just opposite for the BH+ acids. The unionised conjugate base (free amine) is the species most readily crossing the nonpolar membranes, see diagrams for passage of HA and HB+ through lipid barriers
computer-aided drug design: early methods Initially, the design of new drugs was based on starting with a prototypical molecule, usually a natural product and making structural modifications. Examples include steroidal hormones based on naturally occurring cortisone, testosterone, progesterone and estrogen; adrenergic drugs based on epinephrine; local anesthetics based on cocaine; opiate analgesics based on morphine; antibiotics based on penicillin, cephalosporin and tetracycline.
Examples of prototypical molecules that were not natural in origin include the antipsychotic phenothiazines, bisphosphonates for osteoporosis, benzodiazepines indicated for various CNS treatments. Although prototypical molecules have produced significant advancements in treating diseases, this approach to drug development is limited to the initial discovery of the prototypical molecule. Today, it is more common to take a holistic approach that, where possible, involves understanding the etiology of the disease and the structure of the receptor where the ligand (drug) will bind.
Increasing computer power coupled with applicable software, both at reasonable cost, has led to more focused approaches for the development of new drugs. Computational methodologies include mathematical equations correlating structure with biological activity, searching chemical databases for leads and rapid docking of ligand to the receptor. The latter requires 3D structure information of the receptor. Originally crystallized enzymes were the common receptors, and their spatial arrangements determined by x-ray crystallography. Today's software can calculate possible 3D structures of protein starting with the amino acid sequence.
There are many strategies in the design of a drug such that the new drug has a better fit for its desired target binding site. Other strategies involve change in functional groups or substituents such that the drug's pharmacokinetics or binding site interactions were improved. These strategies involve the synthesis of analogue containing a range of substituents. Because there will be a large number of combinations. A rational approach is QSAR.
QSAR attempts to identify and quantify the physiochemical properties of a drug and to check whether any of these properties has an effect on the biological activity. QSAR equations tell about the role of the property on pharmacokinetics or mechanism of drug action. It allows predication of the biologictivity of similar combinations. It also allows, in advance, the calculation of the biological activity of a novel analogue
Because a large number of physiochemical properties may affect the biological activity of a drug and the difficulties involved in quantifying them, a practical approach is to vary one or two properties while keeping the others constant. However, some changes may affect more than one property at the same time. When using QSAR the compounds studied must be related structurally, act on the same target and have the same mechanism of action. In vitro testing of activity is more reliable than in vivo testing due to complications involved.
A graph is drawn of biological activity (log 1/C) versus the physiochemical property e.g log P. The line of best fit through the data points is drawn. Regression coefficients r2 is often quoted with values over 0.8 are considered a good fit. For example a value of r2 signifies that 90% of the drug's activity is accounted for by that property. The larger the number of compounds, the more meaningful r2 will be. It is also common to report the standard deviation ,s, which tells about the experimental error in the physiochemical property determination. It is also a common practice to quote p values derived from F-tests.
A value of p = 0.05 means the parameter is significant otherwise it should not be included in the QSAR equation.
QSAR, Goals Just as mathematical modeling is used to explain and model many chemical processes, it has been the goal of medicinal chemists to quantify the effect of a structural change on a defined pharmacological response. This would meet three goals in drug design: (a) to predict biological activity in untested compounds, (b) to define the structural requirements required for a good fit between the drug molecule and the receptor, and (c) to design a test set of compounds to maximize the amount of information concerning structural requirements for activity from a minimum number of compounds tested.