Download
1 / 25
260 likes | 333 Views
History And Physical. Diane Morris. History of Present Illness.

E N D
History And Physical Diane Morris
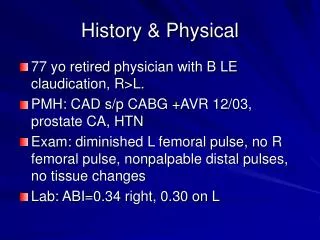
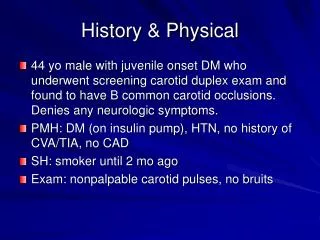
History of Present Illness • Patient is a 60 year old white female who presented to the Emergency Room with complaints of dizziness and “just not feeling right” for a couple of days. Patient states that she was in the car with her male friend they were at a stop light went to turn her vision went blank she became dizzy, and couldn’t hear. Male friend pulled over to the side of the road so she could get her barings. After patient was able to open up her eyes she thought her blood sugar was low ate some candy that she had in her purse and continued to the family function they were going to checking her blood sugar when she got there and it was in the 120’s. Patient stated that she continued to feel “funny” and called her Doctor on Monday for evaluation. Patient was scheduled to have blood work done and outpatient CT for the next day. Patient was still concerned that she was not feeling well on Monday evening, so she went to the Emergency Room for evaluation. Patient was evaluated for possible stroke versus TIA. In the emergency room patient had a CT scan, CXR, EKG and blood work done. CT scan was negative and showed no acute changes, lab values were all within normal limits and CXR showed nothing abnormal.
Past Medical History • Surgical History: • s/p Cholecystectomy 1984 • s/p Appendectomy 1978 • s/p Myxoma Left Atrium 1990 • s/p Left Ear “something removed” 1993
Past Medical History • Medical History: • A-Fib • Type 2 Diabetes • Hypothyroidism • Vertigo • Sleep Apnea, uses CPAP • Anxiety • High Cholesterol
Social History • Patient is divorced lives alone but does have a male friend. Patient does all her own ADL’s, finances and still continues to drive. Has one daughter that lives in the area. Patient denies any use of alcohol, tobacco or illicit drug use. Pt is retired after being a secretary for thirty for years. Pt is a full code.
Family History • Both parents are living. Father has a history of heart disease, cardiac stents, pacemaker, prostate cancer, CABG, and esophagitis and now has to eat pureed food. Mother has a history of HTN, Type One Diabetes, and memory loss with dementia/Alzheimer.
Allergies • Codeine: nausea and vomiting • Iodine and Seafood: rash and hives • Serzone: hallucinations • Celexa: hallucinations • Albuterol: increased heart rate
Medications • Synthroid 188mcg daily-hypothyroidism • Potassium 20 mEq BID • Xanax 0.5mg BID-anxiety • Coumadin 2mg daily-blood thinner • Amiodarone 200mg daily-A-fib • Lipitor 10mg-high cholesterol • Vitamin D 2000iu daily • Zaroxolyn 5mg daily-water pill used for treatment in patients with heart or liver disease • Amaryl 1mg daily-Type Two Diabetes • Lasix 40mg daily-fluid retention
Medications • Glimepride 2mg daily-Type Two Diabetes • Metolazone 5mg daily-water pill used to treat HTN • Tylenol prn • Nasonex prn
Review of Systems • Constitutional: Alert, oriented, skin warm dry and pink, patient is able to answer all questions appropriately, states she has not been feeling well for the last couple of days. • Eyes: PERRLA, denies any changes in vision, only vision change was when episode happened on the car and vision went blank for a second • ENT: Denies any nasal drainage or any changes with hearing, does not wear hearing aids, using Nasonex PRN • Skin/Breast: Denies any rashes, minimal bruising due to medication, no open wounds at time of admission, breast exam not performed
Review of Systems • Cardiovascular: Denies any SOB, CP or chest pressure, irregular heart rhythm (A-fib) which is normal for patient • Pulmonary: Denies any SOB, cough or sputum production • Endocrine: no changes in appetite, pt is taking Amaryl and Glimperide as prescribed • Gastrointestinal: Denies any problems with bowel • Genitourinary: Denies any increase or pain with urination
Review of Systems • Musculoskeletal: Denies any changes in strength, joint tenderness or swelling, no recent falls or trauma • Neurological: Able to answer all questions appropriately, no headache, short and long term memory intact, c/o dizziness with head movement • Psychology: Denies any changes in mood, patient takes Xanax as needed for anxiety • Heme/Lymph: Bruising from medications, no history of DVT or PE, patient is taking Synthroid as prescribed
Physical Exam • Vitals: • Temp 36.6 • Pulse 87 • RR 16 • BP 131/51 • O2 Sat 98% RA
Physical Exam • General: Patient does not appear in any distress, sitting up in bed, eating breakfast • Eyes: PERRLA, EOM intact, no redness or drainage, able to open and close eyes with no difficulties • ENT: No nasal drainage, no difficulty with swallowing, smile equal no drooping, denies any problems with hearing at this time, states at time of incident everything went dark and couldn’t hear • Neck: No redness, swelling or any palpable masses, thyroid not enlarged
Physical Exam • Lymph Nodes: No lymphadenopathy • Cardiovascular: Irregular rhythm (A-fib), RR, no carotid bruits, no JVD • Lungs: Clear to auscultation, no wheezing or use of accessory muscles • Skin: No rashes, skin is warm dry and pink, minimal bruising due to medication • Breast: deferred • Psychiatry: denies feeling anxious, just wants to know if something is wrong • Abdomen: Bowel sounds present in all four quadrants, no pain or tenderness with palpation
Physical Exam • Genitourinary: Genital exam not performed, does not pertain to patients complaint • Rectal: Rectal exam not performed, does not pertain to patients complaint, patient denies any problems with bowels or any blood in stools • Extremities: No edema, clubbing, cap refill <3 seconds, pulses equal bilaterally 3+ • Musculoskeletal: Full ROM all extremities, no edema, no deformities • Neurological: A & O x 3, no slurred speech, no neuro deficits, CN 2-12 intact, moves all extremities with no difficulties
Pertinent Diagnostic Tests • WBC 6.13 • RBC 4.01 • Hgb 12.0 • Hct 31.6 • BUN 23 (result a little high, Lasix can increase level, Diabetic) • Creat 1.2 (normal range but on the high end) • Na 138 • K 4.3
Pertinent Diagnostic Tests • Cl 99 • BiCarb 24 • Caclium 9.0 • CPK 72 • Trop <0.015 • HgA1c 7.3 • Chol 135 • Tri 62 • HDL 70 • LDL 53 • VLDL 12 • TSH 2.5
Pertinent Diagnostic Tests • PT 3-5 25, 3-6 26.1, 3-7 26.1 • INR 3-5 2.4, 3-6 2.5, 3-7 2.5 • UA was neg, no protein in urine
Pertinent Diagnostic Tests • EKG: A-Fib, patient has a history of A-fib, no acute changes since last EKG that is on file • CXR: no infiltrates, no effusions, no acute changes since last x-ray was obtained • CT: no acute changes • MRI: Negative for any acute bleeding or clots, no tumors • Echo with bubble study: normal study, air bubbles followed the normal pathway of the heart • Carotid Doppler: normal blood flow, no evidence of carotid stenosis
Differential Diagnosis • TIA vs. Stroke • Vertigo/Dizziness • Stress Reaction
Impression (final diagnosis) • Vertigo/Dizziness: sensation of motion when there is no motion or an exaggerated sense of motion in response to a given bodily movement, hearing loss is the key to diagnosis for vertigo • Peripheral vertigo: onset of sudden, often associated with tinnitus and hearing loss, horizontal nystagmus may be present • Central vertigo: onset is gradual, no associated auditory symptoms • All tests and lab results came back within normal limits. Patient states that she was feeling better but still had dizziness with head movement.
Plan • MRI • Echo with bubble study • Carotid Doppler • Vestibular Rehab • PT/INR • Lipid Panel
Plan • Patient was admitted to the telemetry floor for continuous monitoring. Orthostatic blood pressures were obtained and showed no difference in laying, sitting or standing. More lab work was obtained for testing lipid levels, HgA1C, and PT/INR daily while admitted to the hospital. More extensive study was ordered: MRI, Carotid Doppler study, and Echo with bubble study. Discharge instructions include following up with PCP in a couple of days, Cardiology in one month and Vestibular Rehab the next day. Instructions also include having repeat lab work done to follow PT/INR. Patient also educated about changing positions slowly, to sit at the end of the chair prior to standing up and sitting on edge of bed before standing. Patient states that her daughter will be able to stay with her for a few days to help take her around to different appointments.
Reflection of Care • After evaluating the patient I talked with my preceptor explained her story and what I thought her diagnosis was and what testing should be done. My preceptor agreed with my diagnosis and ordered what testing I suggested, plus some that he suggested: echo with bubble study and carotid doppler. The main things that I would do differently were to order the other testing and take a bigger look at the picture to think of everything that could be the cause of her dizziness. I did not know though what the echo with bubble study was, so I need to learn about the different types of testing there is to order.