Download

1 / 42
640 likes | 1.89k Views
MANOMETRY Measurement Technique. Jia-Feng Wu, M.D. Division of Gastroenterology, Department of Pediatrics, National Taiwan University Children Hospital. Manometry at NTUH. 1985. 2007. Manometry. Anorectal manometry Esophageal manometry Antroduodenal manometry Oddi sphincter manometry.

E N D
MANOMETRY Measurement Technique Jia-Feng Wu, M.D. Division of Gastroenterology, Department of Pediatrics, National Taiwan University Children Hospital
Manometry at NTUH 1985 2007
Manometry • Anorectal manometry • Esophageal manometry • Antroduodenal manometry • Oddi sphincter manometry
Anorectalmanometry • Indication • Equipment • Preparation • Investigation • Analysis
Anorectalmanometry • Indication • Fecal incontinence • Constipation • Evaluation before-after operation • Equipment • Ano-rectal motility probe • Recording device • Computer • Software
Anorectalmanometry • Equipment • Ano-rectal motility probe • 3, 4, 6 or 8 channels • Balloon • Water perfused • Micro-tip (not very common)
Catheter • Equipment • Ano-rectal motility probe • MicroTip catheter • 1-4 channels • Balloon mounting ring
Preparation • Preparation • Patient must empty bladder and rectum. Enema only needed if patient has severe constipation • Connect catheter to perfusion system • Flush all channels to remove air-bubbles • Zero balance catheter at anal sphincter level • Introduce catheter in Anal sphincter/rectum • Ready to start…...
Investigation • Investigation • Resting/Relax pressure • Squeeze pressure • Endurance squeeze • Push/strain pressures • Cough test • RAIR • Sensation test • Vector Volume/Profile
Resting • Investigation • Resting/Relax pressure • Let the patient rest, no squeeze for 30 seconds • Analyze average resting pressure in the high pressure zone (IAS and EAS)
Squeeze • Investigation • Squeeze pressure • Ask patient to squeeze for about 5 sec • Wait 30 sec and repeat 3 times • Analyze EAS contraction
Endurated squeeze • Investigation • Endurance Squeeze • Ask patient to squeeze for about 25 sec • Analyze fatigue slope of EAS
Push • Investigation • Push/Strain pressure • Ask patient to strain like to defecate • Pitfall: embarrassment of patient • Analyze EAS relaxation
cough • Investigation • Cough test • Ask patient to cough • Analyze EAS contraction in response to sudden increase of abdominal pressure
RAIR • Investigation • RAIR (Recto-Anal-Inhibitory-Reflex) • Inflate balloon (20-50 mL or stepwise 0-10-0-20-0-30-0-40-0-50 with air) • Analyze IAS relaxation and spontaneous EAS response
Sensation • Investigation • Sensation test • Inflate balloon with air stepwise +10 ml (10, 20, 30, 40...250 mL...until Max Vol) • Wait 20-30 sec between inflation for accommodation of the rectum • Ask patient sensation (No sensation, First sensation, urge, max Tolerable volume
Normal data in children J Pediatr Surg 2009;44:1786-90
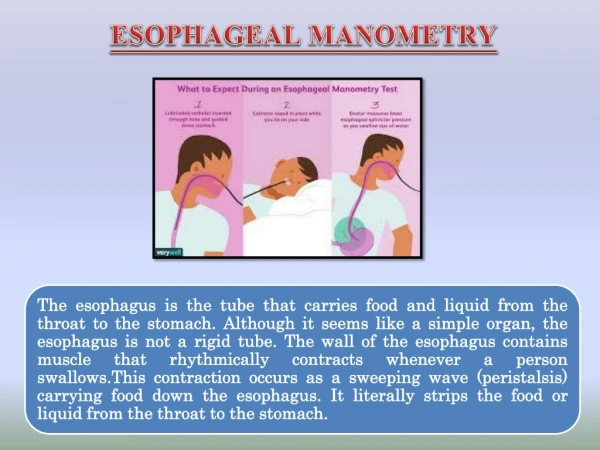
Esophageal manometry • Anatomy • Indication • Equipment • Preparation • Investigation • Analysis
Esophageal manometryindication • Primary esophageal motility disorders • Achalasia • Nutcracker esophagus • Diffuse esophageal spasm • Hypertensive LES • Nonspecific Esophageal motility disorders • Secondary esophageal motility disorders • Scleroderma • Diabetes mellitus • Chronic idiopathic intestinal pseudo-obstruction • Autoimmune disease
Esophageal manometry -indications • Determination of LES prior to pH investigation • Pre-operative to exclude motility disorders for anti-reflux operations • Dysphagia
Catheter • Equipment • Esophageal motility probe • 4-8 channels • 5 cm spacing • Sleeve at the tip
catheter • Equipment • Esophageal motility probe • MicroTip catheter • 3-6 channels
Preparation • Preparation • Patient must fast at least 6 hours • Connect catheter to perfusion system • Flush all channels to remove air-bubbles • Zero balance catheter • Lubricate catheter and introduce via the nose • Ready to start…...
investigation • Investigation • LES: • Gastric baseline pressure • LES resting pressure • LES borders (location) • LES relaxation during swallow • Esophagus: • Esophageal motility (peristaltic contraction) • UES: • Relaxation during swallow
Steps • All channels in stomach; withdraw the catheter stepwise (0.5 cm/withdraw) and mark distances • Look for the lower/upper border of the LES • Position channels in esophagus and LES • Let the patient swallow 10x (dry and wet swallow) • Mark wet and dry swallows • Optional UES
interpretation • Amplitude of primary peristalsis: 48±7 mmHg secondary peristalsis: 46±5 mmHg • Wave onset to peak (promixal): 1.9±0.1 secs (distal): 1.8±0.1 mmHg • Velocity of primary peristalsis: 1.2-2.5 cm/s secondary peristalsis:6.2-7.9 cm/s • Percentage of abnormal wave: < 15% contractions Am J Gastroenterol 2009;104:411-419
Motility disorder • Hypomotility Disorders Achalasia • Hypermotility Disorders Diffuse Esophageal Spasm • Hyperperistalsis Nutcracker • Nonspecific Esophageal Motility Disorders
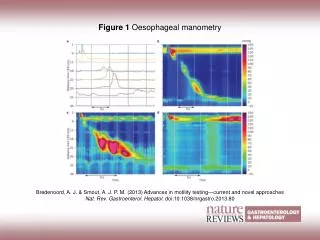
Esophageal spasm Manometry Esophagography
Esophageal spasm • Manometry findings: Peristalsis:>30% abnormal contractions Duration and amplitude occasionally abnormal LES: occasional hypertensive; occasional incomplete relaxation
Achalasia Manometry Esophageography 37
Achalasia • Esophageal manometry findings: normal or increased resting pressure Incomplete or absent relaxation decreased distal contraction amplitude increased resting esophageal body pressure
Nutcracker Esophagus Manometry Esophagography
Nutcracker Esophagus • Manometry findings: Normal peristalsis Contraction amplitude is > 2 SD above normal > 180 mmHg in distal esophagus Duration of contractions >6 sec. LES: occasional hypertensive; usually normal