Download
1 / 13
140 likes | 1.18k Views
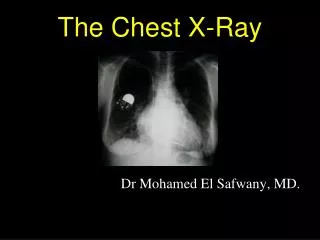
CHEST X-RAY FINDINGS: Left-to-Right Shunt. Uncomplicated ASD: Left-to-Right shunt. enlargement of central and all segments of pulmonary arteries increased pulmonary vascularity , prominent hilar markings “shunt vascularity ”. Uncomplicated ASD : Left-to-Right shunt. RA enlargement

E N D
Uncomplicated ASD: Left-to-Right shunt • enlargement of central and all segments of pulmonary arteries • increased pulmonary vascularity, prominent hilar markings “shunt vascularity”
Uncomplicated ASD: Left-to-Right shunt • RA enlargement • RV enlargement: filling in of retrosternal space; posterior displacement of the LV toward the spine
Uncomplicated ASD: Left-to-Right shunt • RV enlargement: increased opacification posterior to the sternum
Uncomplicated ASD: Left-to-Right shunt • enlargement of the cardiac silhouette • enlarged central and peripheral pulmonary arteries • normal- to small-sized aorta • absent SVC shadow- bec. of rotation of the heart from right-sided cardiac enlargement
Long Standing Shunt • lead to pulmonary arterial hypertension • Eisenmeger Physiology • when pulmonary arterial pressure exceeds systemic arterial pressure, reversal of shunting of blood from left-to-right to right-to-left occurs • CXR findings: • marked central pulmonary artery dilatation • narrowing of peripheral pulmonary artery branches • central pulmonary arteries become aneurysmaland rarely, be calcified
Long Standing Shunt (Eisenmeger Physiology) • enlargement of the right heart • absence of the SVC shadow • aneurysmalenlargement and calcification central pulmonary arteries
Pulmonary Arterial Hypertension • medial hypertrophy, eccentric and concentric intimal fibrosis, recanalized thrombi appearing as fibrous webs, and plexiformlesions • Abnormalities in molecular pathways regulating the pulmonary vascular endothelial and smooth-muscle cells • loss of apoptosis of the smooth-muscle cells allowing their proliferation • emergence of apoptosis-resistant endothelial cells which can obliterate the vascular lumen
Pulmonary Arterial Hypertension • three types of changes in the pulmonary arteries: • Muscular walls of the arteries may tighten up narrower lumen • Walls may thicken as the amount of muscle increases in some arteries. Scar tissue may form in the walls of arteries. As the walls thicken and scar, the arteries become increasingly narrow. • Tiny blood clots may form within the smaller arteries, causing blockages
Pulmonary Venous Hypertension • occurs in the setting of elevated left sided filling pressure • often associated with diastolic dysfunction of the left ventricle; diseases affecting the pericardium or mitral or aortic valves; or rare entities such as cortriatriatum, left atrialmyxoma, extrinsic compression of the central pulmonary veins from fibrosingmediastinitis, and pulmonary venoocclusive disease. • the degree of elevation in pulmonary artery pressure is concordant with the degree of elevation in left atrial pressure.
Pulmonary Venous Congestion • arterialization of the external elastic lamina, medial hypertrophy, and focal eccentric intimal fibrosis • Microcirculatory lesions: capillary congestion, focal alveolar edema, and dilatation of the interstitial lymphatics