Download
1 / 20
240 likes | 857 Views
Tumors of the bile ducts. Gallbladder cancer. Fifth most frequent GI cancer 2 /3 women 75% >65 ani 70-90% associated to litiasis ETIOLOGY Gallbladder litiasis Abnormal bilio-pancreatic junction Porcelain gallbladder Cyst of the main bile duct Sclerozng cholangitis. Gallbladder cancer.

E N D
Gallbladder cancer • Fifth most frequent GI cancer • 2/3 women • 75% >65 ani • 70-90% associated to litiasis • ETIOLOGY • Gallbladder litiasis • Abnormal bilio-pancreatic junction • Porcelain gallbladder • Cyst of the main bile duct • Sclerozng cholangitis
Gallbladder cancer • Pathology • 90% adenocarcinoma • Scquamous cell with small cells, mostly undifferentiated • At diagnosis • 25% limited to the wall • 35% loco-regional metastasis • 40% distant metastasis • 1% incidentally found on apparently normal gallbladders after cholecystectomy • Spread • Lymph – cystic ln – ln near main bile duct – retropancreatic ln – intercavoaortic ln; retroportal ln; coeliac ln. • Direct into the liver • Angiolymphatic along portal tracts • Hematogeneous
TNM Staging for Gallbladder Cancer • T1 Tumor invades lamina propria (T1a) or muscular (T1b) layer • T2 Tumor invades perimuscular connective tissue, no extension beyond the serosa or into the liver • T3 Tumor perforates the serosa (visceral peritoneum) and/or directly invades into liver and/or one other adjacent organ or structure such as the stomach, duodenum, colon, pancreas, omentum, or extrahepatic bile ducts • T4 Tumor invades main portal vein or hepatic artery or invades multiple extrahepatic organs and/or structures • N0 No lymph node metastases • N1 Regional lymph node metastases • M0No distant metastases • M1 Distant metastases • StageStage Grouping • IA T1 N0 M0 • IB T2 N0 M0 • IIA T3 N0 M0 • IIB T1 N1 M0 • T2 N1 M0 • T3 N1 M0 • III T4 Any N M0 • IV Any T Any N M1
Gallbladder cancer • CLINICAL • Can resemble: • Chronic cholecystitis – 40-45% • Acute cholecystitis – 15-20% • Jaundice – 30-35% • Weight loss – 25-30% • Other GI symptoms (upper GI bleeding, bowel obstruction) <5%
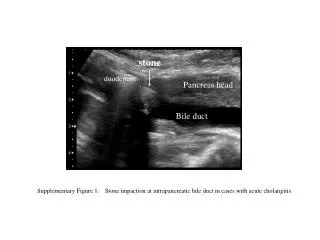
Gallbladder cancer • US • CT, MRI • Echoendoscopy • ERCP • Guided biopsy
Gallbladder cancer • TREATMENT • T1 - cholecystectomy • >T2 - cholecystectomy+lymphadenectomy+hepatectomy with 3-5 cm margin • Unresectable: • Palliative care • Endoscopic or percutaneous stent placing • Radio and chemotherapy – weak chances • PROGNOSIS • 85% die within the first year • 5 year survival • T1a – 100% • T1b – 75% • Std IIa 28-63% • Std IIb 19-25% • Std IV – 1-3 luni
CHOLANGIOCARCINOMA • Rare • W:M=1:1 • 95% adenocarcinoma • Intra- or extrahepatic • Klatskin tumors • ETIOLOGY • Primary sclerotizing cholangitis • Parasites – Clonorchis sinesis • Liver litiasis – 5-10% • Coledoco-duodenal anastomosis
CHOLANGIOCARCINOMA • Symptoms • Variable depending on site and stage • Jaundice • Abdominal pain • Fever, chills • Pruritus • General signs of neoplasia • Palpable gallbaldder • Courvoisier sign
CHOLANGIOCARCINOMA • Diagnosis • Lab • Positive cholestasis tests • CEA, CA 19-9 positive – 40% of patients • Alfa-fetoprotein increased < CH • Imaging • US • CT, MRI
Transhepatic percutaneous cholangiography • Angiography
Treatment • Surgical • Periferal tumor • hepatectomy
Tumor in the hilum • Bile ducts resection + hepatectomy
Tumor of the extrahepatic bile ducts located halfway between the hilum and the papila • Bile duct resection
Tumor of the extrahepatic bile ducts located distally • Bile duct resection + duodenopancreatectomy
Endoscopicaly • Percutaneously • Palliative treatment • Stent placing
CHOLANGIOCARCINOMA • TREATMENT • Photodynamic therapy • Radiotherapy • Unresectable tumors • Chemotherapy • Weak results • PROGNOSIS • 5 year survival • hepatic tumors– 30-40% • perihilar tumors– 10-20% • distale tumors– 40-45% • Unresectable tumors– 5-8 months