Download
1 / 64
650 likes | 798 Views
STI, PID, Genital Tb. Kibruyisfawe zewdie, MD. Sexually Transmitted Diseases. The term denote disorders spread principally by intimate contact:- Sexual intercourse, Close body contact, kissing, and anal intercourse. Transplacental spread, Passage through the birth canal, and

E N D
STI, PID, Genital Tb Kibruyisfawe zewdie, MD
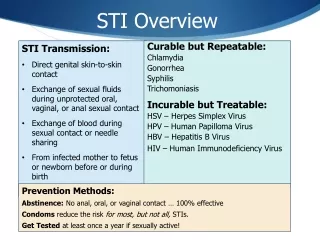
Sexually Transmitted Diseases • The term denote disorders spread principally by intimate contact:- • Sexual intercourse, • Close body contact, kissing, and anal intercourse. • Transplacental spread, • Passage through the birth canal, and • Lactation during the neonatal period
Terminology • WHO recommends that the term STD be replaced by the term STI. • STI has been adopted since 1999 as it better incorporates asymptomaticinfections. • Has also been adopted by a wide range of scientific societies & publications.
Introduction • the most common infectious diseases in the most parts of the world • five key points about all STDs today:
STDs affect men and women of all backgrounds and economic levels. - They are most prevalent among teenagers and young adults. - Nearly two-thirds of all STDs occur in people younger than 25 years of age.
continued 2. The incidence of STDs is rising - Because in the last few decades, young people have become sexually active earlier yet are marrying later. - In addition, divorce is more common. - The net result is that sexually active people today are more likely to have multiple sex partners during their lives and are potentially at risk for developing STDs.
continued 3 Most of the time, STDs cause no symptoms, particularly in women. - When and if symptoms develop, they may be confused with those of other diseases not transmitted through sexual contact. - Even when an STD causes no symptoms, however, a person who is infected may be able to pass the disease on to a sex partner. - recommend periodic testing or screening for people who have more than one sex partner.
continued 4, STDs tend to be more severe and more frequent for women than for men, - because the frequency of asymptomatic infection - many women do not seek care until serious problems have developed. - Some STDs can spread to cause PID, which in turn infertility & ectopic (tubal) pregnancy. - may be associated with cervical cancer; HPV - causes genital warts - other genital cancers.
continued 5. STDs can be passed from a mother to her baby before, during, or immediately after birth; - When diagnosed and treated early, many STDs can be treated effectively. - Some infections have become resistant to the drugs used to treat them and now require newer types of antibiotics.
STD; microorganisms • Long list • Transmitted by sexual route (conventional STI) • Transmission described but less defined evidence
Approaches to STD Dx & Rx Three approaches • Laboratory based • Clinical without laboratory support • Syndromic Approach
Background • Traditional approach to STD Dx and Rx relies on laboratory diagnosis to determine etiologic agents • Expensive • Involves delay in Dx and Rx • Depends on technician and lab accuracy • Often not available in resource poor settings • Requires quality control procedures
…Background • Alternative approach – Clinical Dx • Presumptive Dx of one etiology based on clinical findings • Often inaccurate and incomplete • Similarities of Sn and Sx • Misses Co-infection • Atypical presentation - HIV
Definition • Syndromic Management is a management approach that uses clinical algorithms on an STD Syndrome, the constellation of patient symptoms and clinical signs to determine therapy. • Algorithms are adapted to local STD prevalence • Chooses antimicrobial agents to cover all the possible pathogens responsible for the syndromes in the specific geographic area.
…Syndromic Management Components • Identification and Rx of the Syndrome • Education and counseling on - Rx compliance - Risk reduction including condom use • Partner notification • Provision of condoms • VCT for HIV
Advantages • Expedited care • Cost savings – less technically demanding • Increased client satisfaction • Treatment at first visit • Decreases further transmission • Decreases complication • Eliminates need for return visit • Decrease incidence of HIV (by 42% in Tanzania)
Major STD Clinical Syndromes • Genital ulcer • Urethral discharge • Abnormal vaginal discharge • Lower abdominal pain • Bubo inguinale • Scrotal swelling • Neonatal conjuctivitis
Genital Ulcer Disease (GUD) • Algorithms for GUD try to identify presence of • Herpes, • Syphilis and/or • Chancroid • Frequency of causative agents differ in different parts • Review – syndromic treatment without lab support showed high cure rate • 100% - Cote D’ivore • 64% - Zambia
Herpes Simplex Virus • DNA virus • remain in latent form • other members of the family includes VZ, CMV ,EBV • there are different antigenic strains • but are divided in two:- • Type1 = oral • Type2 = genital • primary infection occurs in child hood • latent infection resides in the sensory ganglion of trigeminal, sacral & vagal • 50 -100% of adults have serologic evidence of HSV1 • 20-80% type2
HSV Cont… • transmission = only by direct contact • clinical disease • painful papule followed by vesicle ,ulceration crusting & healing • more sever in women • Primary Vs Recurrent • primary episode • more symptomatic • incubation range 2-14 days • there is fever & lymphadenities • viral shedding & healing prolonged
HSV Cont… • recurrent episode • frequently have prodromal period signaling active viral replication, • lesions are often localized • shedding is shorter • recurrences is not usually from re infection but are reaction of latent viruses
Diagnosis = mainly clinical • Tissue culture • best method but lengthy and costly • ELISA testing 70% • Direct immunofluoresent staining 75% sensitive = both the negative culture and smear don't exclude infection
Syphilis • organism characteristics & microbiology • By treponema pallidum • is tightly coiled a spirochete that can not be grown • can invade intact mucous membrane or area of abraded skin . • incidence and epidemiology • the incidence is rising • only 30% of patients exposed acquire the disease • in those infected patients not taking medication 60% do develop immune defense sufficient to control the infection • the remaining will go to late and tertiary syphilis
Clinical diseases 1. EARLY SYPHILIS A = primary syphilis, • painless chancre is the whole mark • it occurs at the site of inoculation • there is regional lymphadenopathy • incubation period 10-90 days B = 20 syphilis - mucocutaneous skin lesion 6-8weeks after the original inoculation - alopacia, hepatitis & nephrotic syndrome
continued 2. Latent syphilis • characterized by serologic evidences but no clinical signs &symptoms • most patients are not infectious about 25% could have recent skin lesion • arbitrary division of this stage but has no clinical significance with regard to treatment • early latency (< 4 years from initial infection ) • late latency (>4 years )
continued 3. LATE SYPHILIS • 5-30 years after initial infection • there are three divisions 1. benign disease(gummas) - lesion occur in vital organs • can be life threatening if they compromise the organ 2. cardiovascular disease - involvement of the heart and the aorta are frequent dysfunction may cause serious problem 3. neurological diseases - three clinical syndromes of neurological involvement • asymptomatic disease no neurological manifestations but abnormal CSF • meningovascular disease the commonest manifestation is paresis ,(tabis dorsalis) • parenchymatous disease dementia the commonest manifestation
Diagnosis A. Non treponemal specific test:- • RPR (rapid plasma reagin) test, • standard VDRL slide test, B. Treponemal specific test; • FTA-ABS; fluorescent treponemal antibody absorbed (used commonly for adults ), • MHA_TP micro haemagglutination assay( for neonates) C. Dark field microscopy • the higher the titer the higher the inflammatory reaction • false +ve tests in chronic illnesses • e.g. leprosy - auto immune diseases( lupus) • pregnancy - drug addiction
Chancroid • Haemophilus ducreyi :- a gram negative bacteria • is a painful soft chancre ragged with raised borders • kissing ulcers do occur • unilateral lymphadenopathy that may suppurate • incubation period is 2-5 days • the organism is fastidious
…GUD Genital ulcers Patient complains of genital sore or ulcer Examine -Educate -Counsel if needed -Promote/provide condoms No No Vesicular/recurrent lesion(s) present? Ulcer present? Yes Yes -Treat for syphilis and chancroid -Educate -Counsel if needed -Promote/provide condoms -Partner management -Advise to return in 7 days -Management of herpes -Educate -Counsel if needed -Promote/provide condoms
…GUD • Syphilis • Recommended regimen Benzantine Penicillin 2.4miu im singledose • Alternative regimen Procaine Penicillin 1.2miu im for ten days • Penicillin allergy– TTC 500mg po qid/15d or doxycycline 100mg po bid/15d
…GUD • Chancroid • Recommended regimen Erythromycin 500mg po qid/7days • Alternative regimen Ciprofloxacin 500mg single dose or Ceftriaxone 250mg im single dose or Spectinomycin 2gm im single dose
…GUD • Herpes – to modify course of symptoms • 1st episode – acyclovir 200mg 5x per day /7 days(doesn’t appear to influence natural Hx of recurrent disease) • Recurrence – acyclovir 200mg tid continuously for frequently recurring outbreaks(>6 per year)
Inguinal Bubo • Inguinal adenopathy • LGV (L1,L2,L3), • Chancroid, • G I (donovanosis) is • Klebsiella granulomatis, formerly known as Calymmatobacterium granulomatis • Common in the tropics as a cause of genital ulcer • Men affected more than females • Prostitution is reservoir • Painful adenopathy
Inguinal Bubo, cont’d • Rare systemic symptoms except LGV • Common predisposing factor for the spread of HIV • Complications: • Abscess formation • PID • Lymphatic obstruction • Stenosis • Infertility
Differential Diagnosis • Infection in the lower limbs and perineum • Malignancy • Herpes genitalis • Syphilis
Inguinal Bubo Enlarged and/or painful inguinal lymph nodes? Examine Yes Ulcer(s) present? Use genital ulcers flow chart No -Treat for lymphogranuloma venereum -Educate -Counsel if needed -Promote/provide condoms -Partner management -Advise to return in 7 days
…Inguinal Bubo • Recommended regimen (LGV) Doxycycline 100mg po bid/14 days or TTC 500mg po qid/14 days • Alternative regimen Erythromycin 500mg po qid/14 days or Sulfadiazine 1gm qid/ 14 days • Aspirate fluctuant lymph nodes through normal skin • Incision and drainage or excision of nodes is contraindicated
Vaginal Discharge (VD) • Most difficultsyndrome to diagnose • Either vaginitis or cervicitis • Cervicitis- N.gonorrhea - C.trachomatis • Vaginitis - Trichomonas vaginalis - Candida albicans - Bacterial vaginosis • Effective management of cervicitis is more important from patient point of view b/c of serious sequele
…VD Vaginal Discharge Patient complains of vaginal discharge (vaginal itching) partner symptomatic or specific risk factors positive? No -Treat for vaginal infection -Educate -Counsel if needed -Promote/provide condoms Yes -Treat for cervical and vaginal infections -Educate -Counsel if needed -Promote/provide condoms -Partner management -Return if necessary
…VD Treatment Cervicitis (Gonorrhea & Chlamydia) Recommended regimen Ciprofloxacin 500mg po single dose or Ceftriaxone 250mg im single dose or Cefixime 400mg po single dose or Spectinomycin 2gm im single dose Plus Doxycycline 100mg po bid/7 days or TTC 500mg po qid / 7 days or Erythromycin (pregnant)
…VD Vaginitis Recommended regimen metronidazole 2gm PO single dose or metronidazole 500mg PO bid/7 days plus Nystatin 100,000 IU intra vaginally once/14 d, or Clotrimazole 200mg once daily/3 days, or Clotrimazole 500mg single dose
Lower Abdominal Pain (LAP) Patient complains of lower abdominal pain Take history and examine (abdominal and vaginal) No Follow up if pain persists Temp 38°C or Pain during examination (on moving cervix) or Vaginal discharge No Missed/overdue period or Recent delivery /abortion or Rebound tenderness or Guarding or Vaginal bleeding Yes -Treat for PID -Educate -Counsel if needed -Promote/provide condoms -Partner management Follow up after 3 days or sooner if pain persists Yes Refer No Refer Yes Continue Rx Improved?
PID • PID refers to acute infection of the upper genital tract (above the internal cervical os) • community-acquired Vs Iatrogenic • USA - annually 2.5 million outpatient visits, • 200,000 hospitalizations, and • 100,000 surgical procedures • incurs an annual total expense of more than $5 billion
Acute PID= attributed to an ascending spread of microorganisms from the vagina and endocervix. • Acute PID Vs Acute salpingitis • are often used interchangeably, • but PID is not limited to tubal infection only. • A more descriptive term = (UGTI). • Severity & Extent of disease • This is differentiated from (LGTI) because response to treatment appears to be different in these two entities.
Etiology • Neisseria gonorrhoeae and Chlamydia trachomatis serovars D-K • common cause of PID = 1/3rd each; • However, most = polymicrobial infection caused by ascending infection • 15% of infections occur after procedures that break the cervical mucous barrier • C. trachomatis etiologic role is very different from N. gonorrhea
N. Gonnorrhea Gram-negative IC diplococcus rapid cycle 20 to 40 minutes to divide rapid and intense inflammatory response Less complication Early Rx C.Trachomatis is a slow-growing intracellular organism. lack of mitochondria growth cycle 48 to 72 hours does not induce a rapid or violent inflammatory response destruction by rupture Delayed Rx
Initial PID → • tissue damage provides fertile ground for the growth of secondarily infecting aerobic and anaerobic bacteria. • This necrotic tissue is an excellent growth medium, and • the epithelial damage enhances the breakdown of the surface defense mechanisms
Classification:- • Post STI / menustral • Post abortal • Post Partum • Post Instrumentation • IUD – Related • Secondary PID
Risk Factors 1. STI 2. Age • Adolescent 1:8 Vs 1:80 for a sexually active >24, b/c columnar epithelium 3. Contraceptives • IUDs = threefold to fivefold • Barriers = ↓ 60% • OCP = ↓ risk, good Px fertility • previous tubal ligation = 1/450; 4. Instrumentation ex. 1/200 induced abortion 5. Previous acute PID = 25 %, - partner treatment
Criteria for the Diagnosis:- Major Criteria:- • Cervical motion tenderness or • Lower abdominal / uterine tenderness or • Adnexal tenderness Other minor criteria:- • Oral temperature >101°F (>38.3°C) • Abnormal cervical or vaginal mucopurulent discharge • Presence of abundant numbers of WBC on saline microscopy of vaginal secretions • Elevated ESR • Elevated C-reactive protein • Laboratory documentation of cervical infection with N. gonorrhoeae or C. trachomatis