Download
1 / 36
440 likes | 1.66k Views
Management of Patient with Tracheostomy. Maya Govender Practice Educator – CTICU Foundations of Critical Care (FCCN) 17 th January 2018. Learning Outcomes. List the indications for a tracheostomy List the types of different tracheostomy tubes

E N D
Management of Patient with Tracheostomy Maya Govender Practice Educator – CTICU Foundations of Critical Care (FCCN) 17th January 2018
Learning Outcomes • List the indications for a tracheostomy • List the types of different tracheostomy tubes • List the bed side equipment for a tracheostomy tube • Explain how to decannulate a patient from with a tracheotomy tube • Documentation
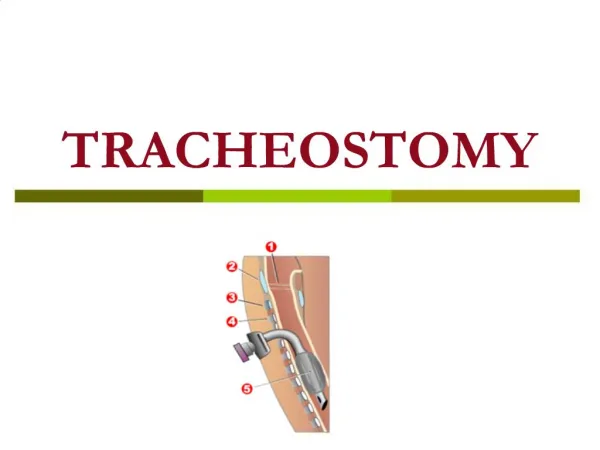
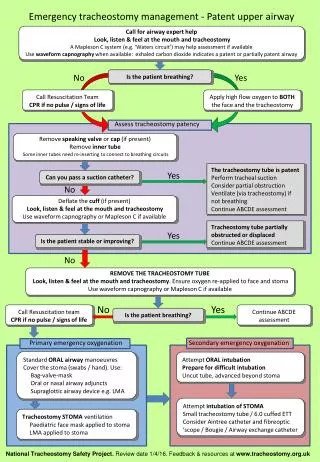
A tracheostomy is an artificial surgically created airway fashion by an hole in the anterior wall of the trachea and the insertion of a tracheostomy tube, which may or may not be permanent What is a Tracheostomy?
Indications • Upper airway obstruction secondary to: trauma, burns corrosive poisoning laryngeal dysfunction foreign body infections, inflammatory conditions obstructive sleep apnoea • Access for pulmonary toilet • Prolonged ventilation support • Airway protection in head injury or comatose patient
Advantages of Tracheostomy • Increased patient mobility • More secure airway • Increased comfort • Improved airway suctioning • Early transfer of ventilator dependent patients from ITU • Enhance communication • Assists in weaning from the ventilator • Decreased risk of pneumonia
How to create a Tracheostomy • Percutaneous Tracheostomy Can be done in the ITU at the bedside • Surgical Tracheostomy • Cricothyroidotomy For urgent procedures
Types of tracheostomy tube used on the unit • Portex blue line without inner tube • Portex blue line ultra with inner tube • Portex blue line ultra fenestrated tube with fenestrated and clear non fenestrated inner tube • Portex blue line adjustable flange tube
Tube sizing ICS, 2008 The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust
Flange 15mm connector Shaft Cuff Obturator Pilot balloon
Cuff Tracheostomy tube • Cuffed tracheostomy tubes: allow airway clearance protect from aspiration positive airway pressure ventilation • It is recommended that cuff pressure be maintained 20 – 25 cmH02
Fenestrated Trachesotomy Tube • The fenestrated tracheostomy tube is similar to the standard tracheostomy tube with the addition of the opening in the posterior portion of the tube above the cuff
Fenestrated Tubes • This allows for assessment of the patient's ability to breath through the normal oral/nasal route • Preparing the patient for decannulation • Patient can talk with the Fenestrated Tube
Longer tubes The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust
Impaired humidification • Increased viscosity of mucus • Depressed ciliary function • Increased risk of infection • Micro-atelectasis • Impaired secretion removal • Obstruction of major airways • Tube blockage • Decreased cough • Infection Presentation title / St George’s University Hospitals NHS Foundation Trust
Humidification • Systemic humidification • Humidify gases • Nebulise • HME and protection from particulate matter The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust
Suctioning • Assessment needed • Reserved for patients unable to clear own secretions • Cough yankeur suction • Pre-oxygenate? • 10-16kPa vacuum • ID mm -2 x2 • Insert 10-15cm, stop if resistance felt and withdraw 2cm The essential principles of tracheostomy care St George’s University Hospitals NHS Foundation Trust
Equipment at the bedside Rebreathe bag, catheter mount, face mask • Ambubag & mask • Working suction, yanker and suction catheters • Tracheal dilators • 2 spare tracheostomy tubes one the same size and one smaller (of the same type of trachy tube in situ) • 10 ml syringe • Clean gloves, aprons and eye protection • Humidification – HME, wet humidification Poster
Care • Inner cannula • Routine use • Inspected four hourly • Cuff • Cuff manometer (20-25cmH2O) • Oral hygiene • Acutely ill patients four - six hourly • Oral fluids where possible The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust
Procedure for cleaning inner tube Wash hands, apply gloves, apron & eye protection • Remove inner tube and replace with the spare inner tube • Rinse the tube through with the sterile water using the disposable bowl • If necessary remove secretions with swabs and rinse with water • Dry with clean gauze • If the inner tube remains soiled and cleaning is ineffective dispose of this inner tube and replace with a new inner tube.
Dressing and fixation The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust
Swallow • Cuff will interfere with swallowing mechanics of larynx • The muscles can waste if not used • Predictors of swallowing difficulty: • Head and neck surgery • Lower cranial nerve palsy • Clinical signs of aspiration • Weak wet or gurgly cough during trials of cuff deflation The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust
Speaking valve The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust
Weaning • Cuff deflation • One way (speaking) valve • Change to a cuffless tube (if needed) • Downsize tracheostomy (if needed) • Capping (if needed) • Decannulation • Airway Patency • Resolved Condition • Effective Cough Strength • Following MDT Discussion The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust
Decannulation of tracheostomy tube Prior to removal patient should: • Be alert and orientated • Have a good cough reflex and managing secretions • Be breathing spontaneously with the cuff deflated • Have a normal respiratory rate, good Spo2 saturations. Check blood gases • Require less than 40 % oxygen via trachy mask • Have anaesthetic review & decision to remove tube agreed with team
Decannulation of tracheostomy tube Ensure all emergency equipment is at hand: • Rebreathe bag, catheter mount & face mask • Ambu bag & mask • Working suction, yanker and suction catheters • Tracheal dilators, 2 spare tracheostomy tubes one the same size and one smaller (of the same type of trachy tube in situ) • 10 ml syringe, clean gloves, aprons and eye protection face mask and oxygen for use following decannulation
Decannulation of tracheostomy tube –(continued) • Ensure cuff is already deflated before removal of tracheostomy • Have emergency equipment attached and ready for use • Connect humidified facial oxygen mask for use after decannulation • Explain the procedure to the patient • Sit patient upright • Suction the mouth and down the tracheostomy tube
continued • Pre oxygenate the patient for 1-2 minutes • Re check respiratory rate, colour and saturations • Remove tube • Place occlusive sterile dressing over stoma • Place oxygen mask on patient • Continue monitoring respiratory rate, saturations and patient colour for any changes.
Post Decannulation Observations The patient should be observed for signs of respiratory distress including: • Dyspnoea • Laboured or noisy respiration, stridor • Increased respiratory rate and heart rate • Excess use of accessory muscles • Diaphragmatic respiration • Agitation • Oxygen desaturation
https://www.stgeorges.nhs.uk/gps-and-clinicians/clinical-resources/tracheostomy-guidelines/https://www.stgeorges.nhs.uk/gps-and-clinicians/clinical-resources/tracheostomy-guidelines/
Presentation title / St George’s University Hospitals NHS Foundation Trust
Documentation • ICP • Type and size of tracheostomy • Tracheostomy procedure • Patent/non patent upper airway • Equipment check • Care record inc. inner cannula, cuff and suctioning • Weaning record The essential principles of tracheostomy care / St George’s University Hospitals NHS Foundation Trust