Download
1 / 20
230 likes | 1.67k Views
Paragonimus Westermani. By Leo Pedretti Elizabeth Hall. Introduction. Causal Agent: Paragonimus westermani also known as the oriental lung fluke. Disease: Paragonimiasis

E N D
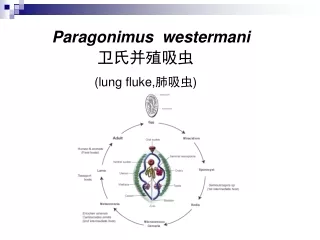
Paragonimus Westermani By Leo Pedretti Elizabeth Hall
Introduction • Causal Agent: Paragonimus westermani also known as the oriental lung fluke. • Disease: Paragonimiasis • More than 30 species of trematodes (flukes) of the genus Paragonimus have been reported to infect animals and humans. Among them, more than 10 species are reported to infect humans, the most common is P. westermani.
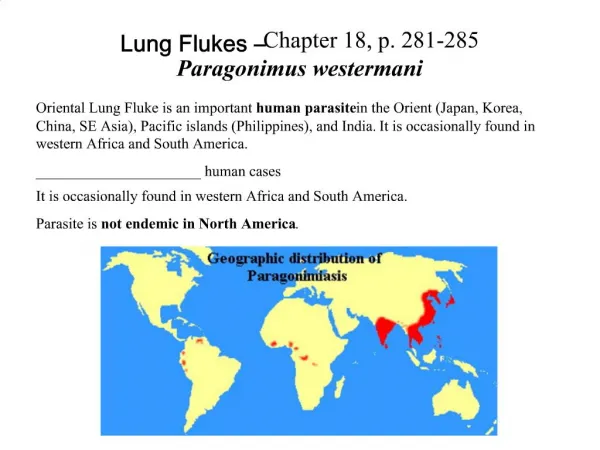
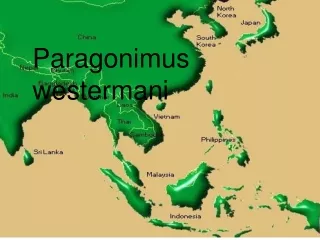
Geographic Distribution • P. westermani infections occur in limited areas where local people eat improperly cooked crustaceans. • P. westermani occurs in the Far East specifically in the countries of Korea, Japan, China, Taiwan, far-east Russia, Malaysia, India, the Philippines, and Indonesia. • Other species of Paragonimus are encountered in Asia, the Americas, and Africa.
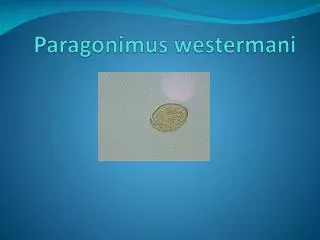
Morphology • The living adult worms are a pinkish-brown color and bean shaped (7 to 15 mm in length to 8 mm in width, and 3 to 5 mm in thickness). It contains a characteristic ovary in the middle of the worm. • The golden brown colored immature eggs are approximately 45-60 μm by 80-100 μm. • The metacercariae in the second intermediate host are spherical in shape measuring 220-450 μm.
Intermediate Hosts • The eggs are passed in sputum or feces. • The eggs flow downstream and have a small chance of survival but this is offset by the fact that the eggs are produced in large numbers. • The miracidium hatches and penetrates its first intermediate host a snail in the family of Thieridae. • In the snail, the miracidium forms a sporocyst that produces rediae, which in turn develop many cercariae. • The cercariae are spined with knoblike tails and minute oral stylets. It is capable of creeping over rocks in inchworm fashion. • It enters its second intermediate host of a crab or crayfish. There are at least 11 different species it infects. Also, there is some evidence that the crabs can be infected by eating snails. • Once in the crab, they encyst in the muscles and viscera.
Definitive Host • The last stage of the parasites development is fulfilled when a mammalian host ingests an infected crab. • Specifically humans, pigs, dogs, and a variety of feline species. • Infections of P. westermani can persist in humans for up to 20 years!
Pathophysiology • When humans ingest raw infected crustaceans, larval flukes develop in the small intestine, penetrate the intestinal wall into the peritoneal cavity 30 minutes to 48 hours after excysting. They then migrate into the abdominal wall or liver, where they undergo further development. Approximately 1 week later, adult flukes reenter from the abdominal cavity and penetrate the diaphragm to reach the pleural space and lungs. Flukes mature, a fibrous cyst wall develops around them, and then egg deposition starts 5-6 weeks after infection. • The symptoms of the early stages of this disease appear to be few with some people being asymptomatic.
Pathophysiology Once the parasite is in the lung or another organ, the worm stimulates an inflammatory response that eventually coats tissue. If worms enter the CSF of the spinal cord, it can result in partial or total paralysis. There have also been fatal cases of Paragonimiasis by infection of the heart. Cerebral cases result in cerebral cysticercosis (condition in which fluid-filled cysts surrounding the worm are present).
Diagnosis • The adult worms can be discovered during surgery or biopsy. • However, it is usually through microscopic examination of the characteristic eggs present in sputum, aspired pleural fluid, feces, and matter of ulcers caused by the parasite. • The eggs may not be present in these sources until 2 to 3 months after infection. • X-ray examination of a pulmonary infection may be mistaken for tuberculosis, pneumonia, spirochatosis, etc. • Cerebral involvement requires differentiation from tumors, cysticercosis, cysts, encephalitis, and others. • Since egg detection rates are low, it would be useful to utilize serological techniques to detect Paragonimus antibodies. • ELISA serological tests are highly sensitive at >92% detection. • Intradermal skin tests performed with an extract of adult Paragonimus is sensitive and hasfew false positives. The results of the skin test may remain positive for up to 20 years after the infection has been cured. • An assay that detects worm antigens with monoclonal antibodies is also available and can be used in conjunction with the intradermal skin test.
Treatment • The most common and effective drug to treat the lung infection is praziquantel. Bithionol is an alternative drug but has more side effects. • The drug is usually taken for 2 days and has a high success rate at or above 95% in the acute phase of infection. • The drug works by increasing cell membrane permeability in susceptible worms, resulting in loss of intracellular calcium, massive contractions, and paralysis of musculature. Produces vacuolization and disintegration of schistosome tegument, followed by attachment of phagocytes to parasite and death.
Treatment • Extrapulmonary lesions may need to be surgically excised. • Intraventricular shunts may also be needed to manage hydrocephalus. • Therapy may also be required for seizures caused by an inflammatory reaction to dying worms in the brain.
Complications • Pulmonary complications include pneumonia, bronchitis, bronchiectasis (bronchial dilation), lung abscess, pleural effusion, and empyema (pus in the plural cavity). • Cerebral complications include seizures and coma. • Skin complications include migratory allergic skin lesions.
Prognosis • The prognosis is good, with therapeutic cure rates between 90 and 100%. • Symptoms resolve rapidly, and eggs disappear from the sputum in a few weeks following treatment. (Pulmonary paragonimiasis may be self-limited, with lesions resolving in 5-10 years in light infections.) • Resolution of abnormalities on chest radiographs may take several months, depending on the chronicity of the disease. • Cerebral infections may be associated with persistent seizures.
Prevention • The spread of the infectious form of this parasite is controlled by cooking freshwater crabs and crayfish until the flesh is pearly and opaque. • Some species of this parasite carrying crab do occur in the Americas and Africa. So, crabs should be cooked everywhere as a general rule.
Pictures The egg form leaves the definitive host and hatches in the miracidium that penestrates the snail. The adult fluke is found in its mammalian host.
Pictures The metacercaria is the form ingested by humans. The cercaria is the form that penetrates the crab.
Questions ~ snails and crabs • 1) What are the intermediate hosts? • 2) What was wrong with the man in the case study report? ~ He had chronic cerebral paragonimiasis resulting in multiple calcified cysts in the brain. • 3) What problems were there with the diagnosis of the man? ~ He had the parasites so long that serological tests showed low antibody levels and no eggs or cysts where found in either stool or sputum. • 4) How do humans contract this disease? ~ By ingesting undercooked or uncooked freshwater crabs or crayfish
References • Centers for Disease Control & Prevention (2004, May 5). Paragonimiasis. [On-Line]. Available: http://www.dpd.cdc.gov/DPDx/HTML/Paragonimiasis.asp?body=Frames/M-R/Paragonimiasis/body_Paragonimiasis_page1.htm. • eMedicane (2006, March 30). Paragonimiasis. [On-Line]. Available: http://www.emedicine.com/ped/topic1729.htm. • Kong, J. (2003). Paragonimus westermani. [On-Line]. Available: http://www.atlas.or.kr/atlas/alphabet_view.php?my_codeName=Paragonimus%20westermani. • Schmidt, G. D., & Roberts, L. S. (2005). Digeneans. In Roberts, L. S., & Janovy, J. Jr. (Eds.), Foundations of Parasitology (7th ed, pp. 279-283). Boston : Mc Graw Hill.