Download
1 / 20
200 likes | 220 Views
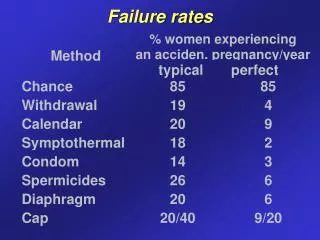
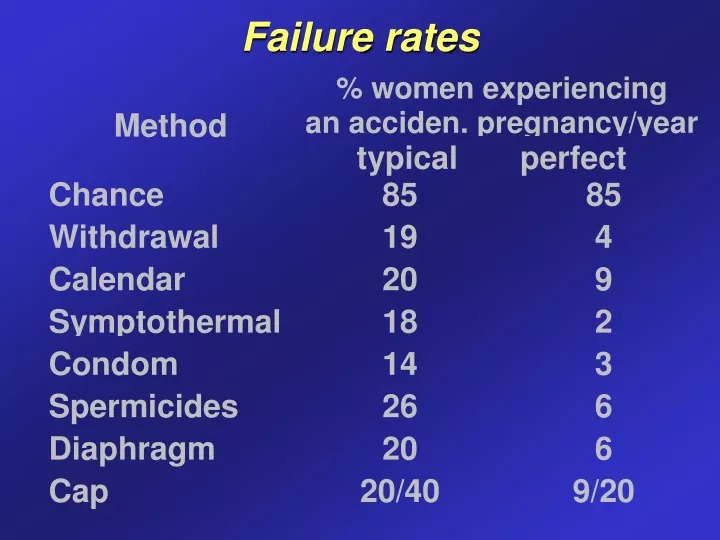
Failure rates. Failure rates. Contraceptive use - USA. Female sterilization 27% OC 26% Male condom 20% Male sterilization 10% Withdrawal 3% Injectable (MPA) 3% Diaphragm 2% Implants 2% IUD 1%. Natural family planning.

E N D
Contraceptive use - USA • Female sterilization 27% • OC 26% • Male condom 20% • Male sterilization 10% • Withdrawal 3% • Injectable (MPA) 3% • Diaphragm 2% • Implants 2% • IUD 1%
Natural family planning • identification of potentially fertile days + periodic abstinence • calendar - assumption: • ovulation on day 14 (± 2) of menstrual cycle • sperm viability 5 days • oocyte viability 24 hours • abstinence days 9-15 (7-17) • failures even with regular cycles, does not account for additional factors (stress, illness, travel) • does not work well for women with irregular cycles, chronic cervicitis/vaginitis
Natural family planning • BBT method: daily temperature readings; temperature rise by 0.4 C/F after ovulation • Cervical mucus (Billings) method: observation of the cervical secretions: fertile days - increase in secretions that are clear , strechy and slippery • Symptothermal method: combination of the fertility indicators (cervical mucus, BBT and/or calendar) Home ovulation detection kits (urinary LH)
Lactational amenorrhoea method • Baby less than 6 months • Amenorrhoea since lochia ceased • Fully or nearly fully breastfeeding 2% chance of pregnancy
Barrier methods • Male condom (latex, polyurethane) • Female condom (polyurethane Reality) • Diaphragm (6h/6h, not longer than 24h TSS, UTI) • Cervical cap (up to 48h, spermicide necessary, Prentif cap) • Spermicides (films, gels, foams, suppositories; nonoxynol-9 2-12%- surfactant that destroys cell membrane; protective against STI)
IUD • With copper (Copper T380): • sterile, inflammatory, hostile endometrial environment • inhibits sperm migration • inhibits fertilization and oocyte transport • With LNG (Mirena): as above PLUS • thickens cervical mucus • augments atrophic decidualization of endometrium • ? may inhibit ovulation
IUD • Appropriate selection • Contraindications: • acute PID / history of PID • genital bleeding of unknown etiology • known/suspected uterine or cervical malignancy • decreased immunoresistance (leukemia, AIDS) • allergy to copper • distortion of the uterine cavity • multiple sex partners
IUD • NOT an abortifacient • DOES NOT increase the risk of ectopic (actually decreases the risk) • DOES NOT increase the risk of PID • DOES NOT increase the risk of subsequent infertility • DOES NOT increase the risk of cervical and uterine cancer
DMPA injections • IM injection every 3 months (150mg of DMPA) • blocks LH surge and prevents ovulation • side-effects: menstrual changes (irregular bleeding , amenorrhoea)
Subdermal implants • Norplant I : 5 year LNG implant system (six tubes; 85ug of LNG daily, by year 5 30ug) • Norplant II (Jadelle) : 3 year 2 rod system • Implanon : (single implant with 3-keto-desogestrel, 3 year) • side-effects + difficulties with removal
Combined oral contraceptives COC • 20-50 ug of EE • progestin: • desogestrel, norgestimate, gestodene • LNG, Norethisterone (NET, NETA) • monophasic : constant dose of E and P • biphasic and triphasic : mainly variation of P dose (also E dose possible) • used by 30-40% of reproductive age women in Western Europe
Combined oral contraceptives COC • prevent ovulation by suppression of pituitary LH/FSH secretion • additional P effects: • changes in the cervical mucus hindering sperm transport • changes in the endometrium: prevention of implantation • decreased tubal motility : delayed oocyte transport
COC - health benefits • Ovarian cancer: risk reduction by 40-80% • Endometrial cancer: risk reduction by 50% • Benign breast conditions ( risk) • PID ( risk) • Ectopic pregnancies ( risk) • Functional ovarian cysts ( risk) • Menstrual effects: improvement in regularity + anemia + dysmenorrhea • Bone density • Acne
COC - health risks • Breast cancer: small or no increase • Cervical neoplasia: increase in cervical adenocarcinoma, does not increase the risk of invasive cervical cancer • VTE: 2-3 fold increased risk (0.4 to 1.0 per 10.000 women, but in pregnancy 6 per 10.000) • MI: no increase in the risk (only for the smokers > 35 years) • stroke: no increase in the risk with low dose COC in nonsmoking women
COC - contraindications • Appropriate selection • Contraindications: • thromboembolic disorder (active or past) • coronary artery/ cerebral vascular disease • carcinoma of the breast • carcinoma of the endometrium or other estrogen-dependent neoplasia • active hepatic disease • pregnancy • smoking after 35 years of age
COC - side effects • nausea • bloating • menstrual changes • breast tenderness • ?? headache • ?? weight gain
Progestin only pills (POP) • Indications - can not tolerate E or contraindications: • breastfeeding women • postpartum women • older women with CVD • women at increased risk for VTE • NET or LNG • no delay (even hours not allowed) in administration
Emergency contraception • Immediate IUD • Yuzpe method: 72h, efficacy max. 24h; 2 pills 250ug LNG + 50ug EE (Ovran) followed by further two tablets 12 hours later • LNG alone (POEC): 750ug LNG stat and 750ug LNG 12h later; 72h, efficacy max. 24h; more effective than Yuzpe, fewer side effects (nausea+vomiting)