Download
1 / 97
970 likes | 991 Views
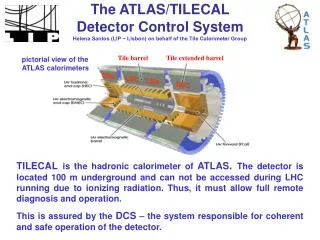
Implementation of evidence-based chiropractic (EBC) in everyday practice can help practitioners in solving clinical questions and making informed decisions for patient management.

E N D
Evidence-based chiropractic (EBC) in everyday practice Implementation of EBC
EBC has many uses • The steps of EBC were intended for use in solving clinical questions • They are also useful to help practitioners answer many other types of questions • e.g., which continuing education seminars to attend, educational materials to purchase, or equipment to purchase Evidence-based Chiropractic
A 23-year-old female patient with neck pain & headache • Headache • Frequency 3-4 per week, lasting 3 to 4 hours • Extends from behind the right eye to the occiput • No aura • Reclining in a darkened room at the onset limits the pain to 4 on the 11-point NRS; if not, may become 8 or 9 with nausea and vomiting • Headache Disability Inventory score is 55 Evidence-based Chiropractic
Neck pain & headache patient (cont.) • Neck pain • Constant • Intensity varies from 2 to 9 on the NRS • Trigger points with grade 2 tenderness are present in the upper cervical region • Cervical ROM restricted and painful on extension and lateral bending bilaterally • Characteristic Pain Intensity score is 6 Evidence-based Chiropractic
Neck pain & headache patient (cont.) • Medication does not really help, so she wants to try chiropractic • How should one proceed in this case? • Is chiropractic care for migraine headache evidence-based? • Are there adjunctive therapies that may be beneficial? • Does the patient have migraine versus cervicogenic headache? Evidence-based Chiropractic
Create a clinical question • Background question • What is migraine and how is it different from cervicogenic headache? • Headache that lasts 4 to 72 hours, is throbbing, is moderate to severe in intensity, is unilateral, becomes worse with exertion, and is associated with nausea, vomiting, or sensitivity to light, sound, or smell • Clinical question • What diagnostic tests can differentiate migraine from cervicogenic headache? Evidence-based Chiropractic
Create a clinical question (cont.) • Foreground question • Is spinal manipulation effective at reducing headache in a young adult female patient? • Patient or Problem:ayoung adult female headache patient (P) • Intervention: manipulation(I) • Comparison: tests that can differentiate migraine from cervicogenic headache (C) • Outcome: reduced pain (O) Evidence-based Chiropractic
Select search terms • Choose several key words from the clinical question • e.g., migraine or cervicogenic headache • Search the MeSH Database for migraine to find MeSH terms • Migraine without aura is most appropriate • There are no MeSH terms for cervicogenic headache Evidence-based Chiropractic
Search MeSH from PubMed Or search from the MeSH Database Evidence-based Chiropractic
Search the databases • PubMed is searched using Cervicogenic headache as a text word • The final search terms are as follows migraine without aura AND cervicogenic headache [tw] • 19 items result, with an article by Antonaci et al. being particularly relevant • But it does not discuss treatment Evidence-based Chiropractic
Search (cont.) • A text word search is performed using cervicogenic headache without the MeSH term and limits set to “Meta-analysis” • An article by Bronfort et al points to a positive effect with manipulation equivalent to commonly used prescriptions and better than massage • The other article is on electrotherapy, but does not point to effectiveness Evidence-based Chiropractic
PubMed text word search Limits are set to meta-analysis Evidence-based Chiropractic
Search the databases • A search of the MANTIS database using the same search terms with the “High Clinical Relevancy” option checked produces 21 citations • A systematic review by Astin and Ernst conflicts with Bronfort et al. • However, numerous errors and omissions were pointed out in a Letter to the Editor • Thus, the Bronfort meta-analysis is chosen Evidence-based Chiropractic
MANTIS search terms High Clinical Relevancy checked Evidence-based Chiropractic
Search (cont.) • Another study points to a dose-response relationship between chiropractic care and cervicogenic headache • Larger doses (9 to 12 chiropractic treatments) were more beneficial than lower doses * Haas, M., et al., Dose response for chiropractic care of chronic cervicogenic headache and associated neck pain: a randomized pilot study. J Manipulative Physiol Ther, 2004. 27(9): p. 547-53. Evidence-based Chiropractic
Critique the articles found in the literature search • Appraise the Bronfort et al. systematic review using an appropriate checklist • The review appears to be valid • Its methodology was sound • A thorough search was carried out • Articles were accurately appraised and synthesized in an unbiased manner Evidence-based Chiropractic
Apply the evidence from the articles • Apply the information to the management of the patient’s condition • Consider the practitioner’s clinical expertise and the patient’s values • Chiropractic adjustments are recommended • Visit frequency is 3 times per week • OMs will be re-administered at 2 and 4 weeks Evidence-based Chiropractic
Patient values • The patient is hesitant to accept cervical manipulation because of the stroke risk • However, she ultimately accepts the treatment recommendations • When informed that the risk is 1 per 1,000,000 cervical manipulations or less • And that these types of strokes have been reported following many other activities involving neck movement Evidence-based Chiropractic
Review the efficiency of the first 4 steps of EBC • The PubMed search may have been too limited because so few citations were retrieved • The statement about the incidence of stroke following cervical manipulation was not evidence-based • Another investigation should be done to verify the statement’s accuracy Evidence-based Chiropractic
Cervical manipulation and stroke search • PubMed search strategy chiropractic manipulation AND (stroke OR dissection) AND incidence • 16 citations result • Mostly case reports and review articles • Incidence estimates show the rate of stroke reports to range from 1:400,000 to 1:5,846,381 cervical manipulations • Hence, the 1:1,000,000 estimate is probably correct Evidence-based Chiropractic
Selecting postgraduate education • Countless seminars, conferences, and meetings are available • Some are very high-quality, some are very poor-quality • Which ones are likely to be useful? • Evidence-based methods are the best way to evaluate them Evidence-based Chiropractic
Factors to consider about postgraduate education • Is it affiliated with a trustworthy sponsoring organization like a chiropractic college or association? • Affiliation is not a guarantee that the material is valid and worthwhile, but it is more likely since basic requirements must be met • Lecture notes and other material should be critiqued using strategies similar to those used to evaluate journal articles Evidence-based Chiropractic
Factors to consider about postgraduate education (cont.) • Instructors should have legitimate credentials and specialties in the topic • Beware of inflated or falsified credentials • Diplomate status should be from a recognized and credible specialty organization • Do a literature search see if the speaker has been published • Were the journals peer-reviewed? Evidence-based Chiropractic
Factors to consider about postgraduate education (cont.) • Unconventional terms should be adequately defined • The use of nonstandard terminology is a red flag for untrustworthy information • Consider another seminar if these criteria are not met • Evidence-based methods can also be used to evaluate seminars after attending them Evidence-based Chiropractic
Green’s criteria to evaluate chiropractic techniques • Is there a reasonable anatomic and physiological basis for the procedures involved? • Is research available on the treatment and/or diagnostic methods? • Is literature available that covers indications and contraindications to the procedure? Evidence-based Chiropractic
Green’s criteria to evaluate chiropractic techniques (cont.) • Is a reliable test available to measure clinical change? • Is the procedure’s response reproducible? • Is the procedure cost effective? • Learning experiences are better when interactive, with adequate time for Q&As Evidence-based Chiropractic
Dr. DA Versendaal has been developing and researching CRA for over 40 years . . . Evidence-based Chiropractic
The American Chiropractor Evidence-based Chiropractic
1998 Evidence-based Chiropractic
Scientifically and clinically proven. Evidence-based Chiropractic
1998 Evidence-based Chiropractic
Equipment purchases • There are many possible choices • Wrong choices waste money and may be useless or even potentially harmful to patients • Sometimes manufacturers claims are misleading • Examples • “Clinically proven” • “96% success rate” • “Established reliability” Evidence-based Chiropractic
Equipment purchases (cont.) • The validity and reliability of diagnostic equipment can be assessed by searching the literature to find studies that have tested the equipment • Although the specific brand name may not be mentioned, but the underlying theory has been tested • A comparable version of a previously validated instrument may not need testing Evidence-based Chiropractic
Sometimes studies disagree • For instance, the Scoliometer • Several studies have investigated its reliability and validity, but conclusions have been conflicting • Cote et al. reported that the interexaminer measurement error of the Scoliometer was high • They felt that the Adam’s forward bending test was more sensitive than the Scoliometer Evidence-based Chiropractic
Studies disagree (cont.) • The authors concluded that the Scoliometer is not appropriate for independent use as a diagnosis or patient management tool because of its poor validity • However, another study showed it to be suitable for screening purposes • One may need to read several articles, or a good systematic review, to discover the worth of a diagnostic device Evidence-based Chiropractic
Thermocouple devices • Used to measure side-to-side paraspinal temperature differences • When temperature variation occurs over a spinal segment, it is thought to represent neurophysiologic dysfunction caused by vertebral subluxation • However, their validity has been questioned and little research exists to support their use Evidence-based Chiropractic
Thermocouple devices (cont.) • Clinical question • Is the assessment of paraspinal temperature via thermocouple devices valid and reliable? • Search terms for use on the PubMed and ICL databases • Thermocouple, nervoscope, and neurocalometer • Thermocouple produces nearly 800 citations using PubMed (too broad) Evidence-based Chiropractic
Thermocouple devices (cont.) • Only 11 citations are produced when the term is combined with spine using the AND operator • Neurocalometer retrieves only one article that discusses the instrument from a historical perspective • Searching ICL for thermocouple returns one article, neurocalometer three, and nervoscope zero Evidence-based Chiropractic
Thermocouple devices (cont.) • 3 articles were retrieved that might be helpful • They must be evaluated for quality and to determine if they contain relevant information • A literature review reported that the reliability of thermocouple devices was supported by a study by Plaugher et al. • Its methodology should be critiqued using an appropriate checklist Evidence-based Chiropractic
Plaugher et al. • Compared the findings of Nervoscope scans of the cervical-thoracic, mid-thoracic, and lower lumbar regions for intraexaminer and interexaminer reliability • Data from the lumbar spine were not analyzable and cervical-thoracic interexaminer reliability was weak • However, good interexaminer agreement was reported in the mid-thoracic spine Evidence-based Chiropractic
Plaugher et al. (cont.) • Examiners were considered to agree when both recorded a positive finding anywhere within the 5 mid-thoracic vertebrae • Yet, most chiropractors apply spinal adjustments to specific levels • It is questionable as to how relevant these findings are to clinical practice • A later review indicated that there were many unresolved questions about these devices Evidence-based Chiropractic
Plaugher et al. (cont.) • Several other problems with this study • The study sample consisted of healthy chiropractic students that were selected out of convenience • Good validity/reliability studies are selected from a defined population that has the same spectrum of disease severity as is seen in clinical practice • No demographic data were presented • Needed to assess the makeup of the sample Evidence-based Chiropractic
Plaugher et al. (cont.) • A funding source was the Gonstead Clinical Studies of Society, which promotes the use of this device • A possible conflict of interest • Based on this evidence, should a practitioner purchase one of these devices? Evidence-based Chiropractic
Thermocouple devices (cont.) • Armed with the knowledge obtained from this evidence-based process, one can now make an educated decision • Very little evidence supports its validity or reliability • Few studies have dealt with the topic and those that have are unconvincing • Practitioners should therefore choose other established diagnostic methods Evidence-based Chiropractic
Thermocouple devices are used by many practitioners • Their use is part of an adjustive technique system that is utilized by more than 50% of chiropractors in the United States • In the face of ambiguous evidence, one could still opt to use a thermocouple device as an aid to spinal analysis • However, it should be used alongside other valid tests Evidence-based Chiropractic
When evidence is lacking for your topic • Unsystematic observations or a generalization from a physiological study will be available for any topic • But this type of evidence is extremely weak • Practice guidelines may help, but are not always available and may be inconsistent • Therefore, other methods are required to help guide decisions about patient care Evidence-based Chiropractic