Download
1 / 18
180 likes | 369 Views
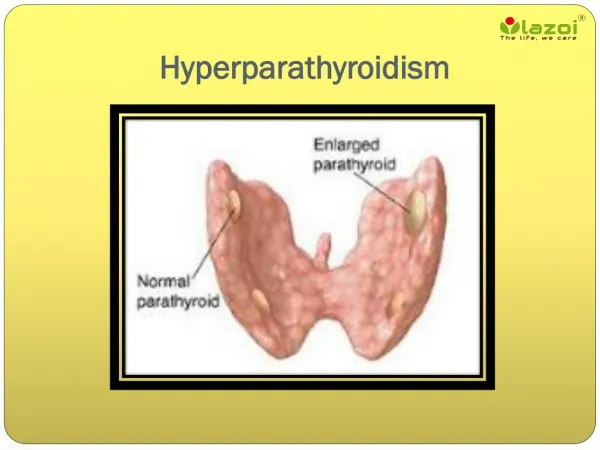
Hyperparathyroidism. overactivitiy of the parathroid gland PTH strong osteoclastic hormone Primary parathyroid gland adenoma Secondary chronic renal disease Hemodialysis (endstage renal glomerular disease) aka renal osteodystrophy. Primary HPT. most common type

E N D
Hyperparathyroidism • overactivitiy of the parathroid gland • PTH strong osteoclastic hormone • Primary • parathyroid gland adenoma • Secondary chronic renal disease • Hemodialysis (endstage renal glomerular disease) • aka renal osteodystrophy
Primary HPT • most common type • mc cause of hypercalcemia • parathyroid adenoma 90%) • carcinoma, hyperplasia, ectopic PTH producing tumors • elevated parathormone levels, hypercalcemia, hypophosphatemia
Secondary HPT • complication of chronic renal disease • persist loss of calcium and phosphorus • stimulates PTH release (high PTH and low to normal calcium) • Hyperphosphatemia (kidneys can’t excrete it as well) • Tertiary HPT is seen in dialysis patients, parathryoid gland acts independent of serum calcium levels (high PTH and Calcium) • Radiographic DDx of types is difficult
30-50 women > men • bone pain, fractures, weakness, lethargy, polydipsia, polyuria • Hypercalcemia leads to muscle weakness, hypotonia • may have renal stones • pancreatitis • hypercalcemia in primary, normal to low in secondary • elevated alkaline phosphatase • elevated PTH
stones, bones, abdominal groans and psychiatric moans (renal stones, peptic ulcers, pancreatitis, confusion, lethargy, weakness)
Parathormone physiology • maintains the circulating level of calcium ion • stimulates osteoclasts, which reabsorb bone and release calcium and phosphorus ion into the blood stream • increase calcium absorption through the small intestine • renal tubular phosphate excretion and calcium absorption; upsets homeostasis • in secondary HPT; calcium loss and abnormal Vit D formation leads to hypocalcemia and release of PTH
Radiography - HPT • Osteopenia • Subperiosteal resorption (diagnostic) • Distal tuft resorption • Accentuated trabeculation • Brown tumors (cystic accumulations of fibrous tissue) • Loss of cortical definition • Soft tissue calcification • Metastatic calcification; eg., vascular calcification
Subperiosteal resorption • most definitive radiographic sign of HPT • esp at the radial margins middle and proximal phalanges of the 2nd and 3rd digits • outer cortical erosion may appear frayed or lace like • widened joint spaces and osteolysis, esp AC and SI joints
Rugger Jersey spine Sub-endplatesclerosis
Undifferentiated seronegative spondyloarthropathy (history, clinical presentation and what is the most likely