Download
1 / 82
820 likes | 840 Views
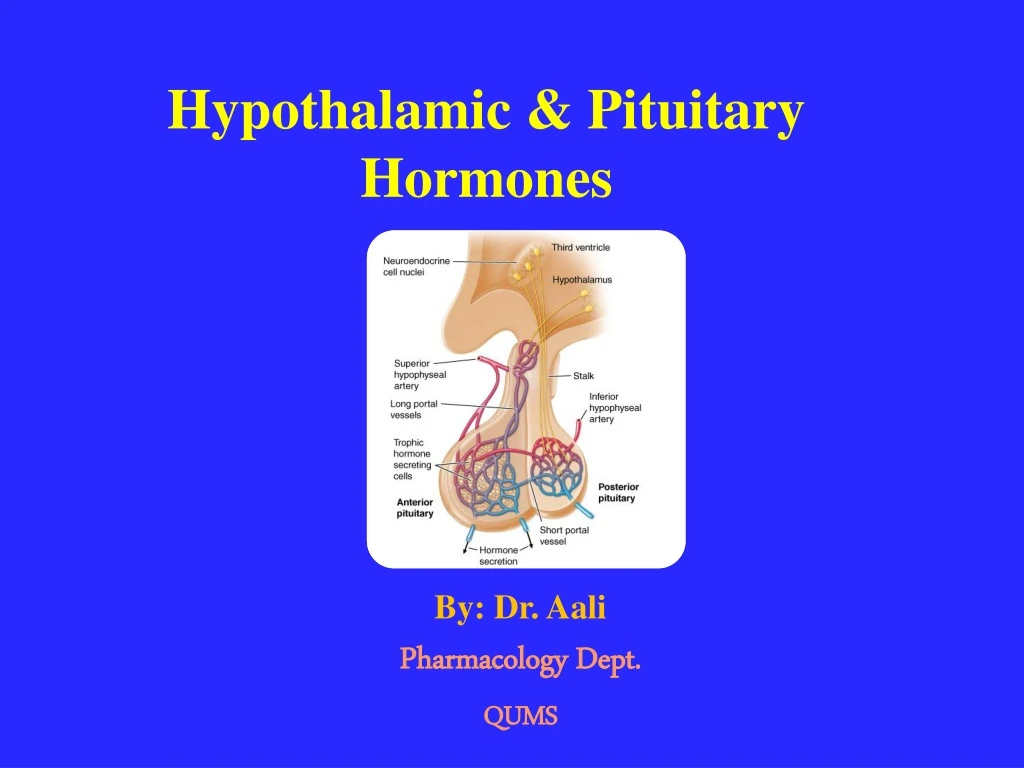
Hypothalamic & Pituitary Hormones. By: Dr. Aali Pharmacology Dept. QUMS. Hypothalamic-Pituitary-Endocrine Axis. Many of endocrine hormones (e.g., cortisol, thyroid hormone, sex steroids, GH) are regulated by mutual interactions among hypothalamus-anterior pituitary-endocrine glands.

E N D
Hypothalamic & PituitaryHormones By: Dr. Aali Pharmacology Dept. QUMS
Hypothalamic-Pituitary-Endocrine Axis • Many of endocrine hormones (e.g., cortisol, thyroid hormone, sex steroids, GH) are regulated by mutual interactions among hypothalamus-anterior pituitary-endocrine glands.
Pituitary Hormones and Their Hypothalamic Releasing Factors • Anterior pituitary hormones are essential for regulation of growth and development, reproduction, response to stress, and metabolism. • Synthesis and secretion are controlled by: • Hypothalamichormones • Hormones from peripheral endocrine organs • A large number drugs affect their secretion. • Synthetic peptide agonists and antagonists have important diagnostic and therapeutic applications.
Anterior Pituitary Hormones Classification • Anterior pituitary hormones classified into three different groups based on their structural features: • Somatotropic hormones: • Growth hormone (GH) • Prolactin(PRL) • Glycoprotein hormones: • Luteinizing hormone (LH) • Follicle-stimulating hormone (FSH) • Human chorionic gonadotropin (hCG) • Thyroid-stimulating hormone (TSH) • POMC-derived hormones: • Corticotropin (ACTH)
Receptors • TSH, FSH, LH, hCG, ACTH activate GPCR. • GH and prolactin act via cytokine receptor family.
Posterior pituitary gland • The posterior pituitary gland, also known as the neurohypophysis. • Contains the endings of nerve axons arising from neurons in SON and PVN of hypothalamus. • Synthesize Arginine vasopressin(AVP: AHD) andOxytocin. • AVP plays important role in water homeostasis. • Oxytocin plays important roles in labor and parturition and in milk letdown. • Both receptors: GPCR
Somatotropic Hormones: • Growth Hormone • Prolactin
Growth Hormone and Prolactin • Structurally related members of somatotropic hormone family. • Pituitary cells that produce GH and prolactin, are somatotropes and lactotropes. • Have structural similarities • GH and prolactin act via membrane receptors belong to cytokine receptor family. • Both hormones activate JAK/STAT
Negative Regulation of secretion • The secretion of both hormones is subject to strong inhibitory input from hypothalamic neurons. • Prolactin: negativedopaminergicinput • GH: negativesomatostatininput
Growth Hormone (Somatotropin) • GH is 191-amino-acid peptide. • Single polypeptide chain of 22 kDa. • Produced by GHRH. • By binding to GPCR on somatotropes, Stimulates GH secretion. • Its major peripheral effector, insulin-like growth factor 1 (IGF-1: somatomedin C). • Act in negative feedback loops to suppress GH secretion.
Physiological Effects of GH • Stimulation of longitudinal growth ofbones. • Increases bone mineral density after the closure of epiphyses • Differentiationofprechondrocytes to chondrocytes • Differentiation of preadipocyteto adipocytes. • Stimulation of osteoclast and osteoblast proliferation. • Stimulation of myoblast differentiation and increased muscle mass. • Increased glomerular filtration rate.
Physiological Effects of GH • Anti-insulin actions: decrease glucose utilization and increase lipolysis. • Stimulate gluconeogenesis. • Development and function of immune system. • Increase lipolysison adipocytes. • Anabolic and growth-promoting effects.
GH Disorders • GH Deficiency (Dwarfism /Nanism/Short stature) • Children GH Deficiency • GH Deficiency • GHRH Receptor Mutations • Growth Hormone Insensitivity • Nutritional Short Stature • Psychosocial Short Stature • Adult GH Deficiency (AGHD) • Hypothalamic or pituitary somatotropedamage • GH Excess (Acromegaly/Gigantism) • Somatotropeadenoma • Extrapituitarylesions
Pharmacotherapy of Disorders of GH
Pharmacotherapy of GH Deficiency • Recombinant Human Growth Hormone (Somatropin) • Rx: Genotropin, Humatrope, Norditropin, Nutropin, Omnitrope • Insulin-Like Growth Factor 1 (IGF-1) • Rx: Mecasermin (Increlex)
Growth Hormone • Recombinant human GH (rhGH) consists entirely of 22 kDa form. • Somatropinhas 191-amino-acid sequence that is identical with native form of human GH • Abuse for sports performance enhancement(which is detected by test)
Pharmacodynamics of GH • GH mediates its effects via JAK/STAT cytokine receptor superfamily. • The growth-promoting effects are mediated principally by increase in production of IGF-I. • Much of the circulating IGF-I is produced in the liver. • GH also stimulates production of IGF-I in bone, cartilage, muscle, kidney, and other tissues, where it plays autocrine or paracrine roles.
Pharmacokinetic • Predominantly cleared by liver. • rhGHis administered subcutaneously 6–7 times per week. • Recombinant GH (0.02–0.05 mg/kg per day)
(Extra Content)Usual Pediatric Dose • Genotropin and Omnitrope:0.16 to 0.24 mg/kg/week, subcutaneously divided into equal doses given either 6 or 7 times a week. • Humatrope:0.18 mg/kg per week, subcutaneously divided into equal doses given either on alternate days or 6 times a week. Norditropin:0.024 to 0.034 mg/kg/day, subcutaneously 6 or 7 times a week. • Nutropin and Nutropin AQ:0.3 mg/kg per week subcutaneously divided into daily injections. In pubertal patients, dosage may be increased to 0.7 mg/kg per week • NutropinDepot:1.5 mg/kg subcutaneously once a month.Patientsmore than 15 kg will require more than one injection.
Clinical Pharmacology • Growth Hormone Deficiency • Pediatricpatients withShort Stature (Turner syndrome, Noonan syndrome, Prader-Willi syndrome) • Treatment of wasting in patients with AIDSand Cachexia • Treatment of patients with short bowel syndrome (intestinal resection) • GH is a popular component of “anti-aging” programs • By athletes for increase in muscle mass and athletic performance (banned by the Olympic Committee)
Side Effects • Hypertension • Tachycardia • Edema • Headache, insomnia • Gynecomastia • Arthralgia, Myalgia • Acne, rash, nevus growth • Upper respiratory tract infection, rhinitis, bronchitis • Otitis media, Pharyngitis • Nausea, Vomiting, Gastroenteritis, Dyspepsia • Hyperglycemia, Hypothyroidism, Hyperlipidemia, • Pancreatitis
Serious adverse effects in children include • Pseudotumorcerebri • Slipped capital femoral epiphysis • Progression of scoliosis • Edema • Hyperglycemia
Insulin-Like Growth Factor 1 (IGF-1)
Insulin-Like Growth Factor 1 (IGF-1) • IGF-1, somatomedin C, is a protein encoded by IGF1 gene. • Binding to its receptor, IGF1R, a tyrosine kinase receptor. • Stimulates systemic body growth. • Has growth-promoting effects on most of cells, especially skeletal muscle, cartilage, bone, liver, kidney, nerves, skin, hematopoietic cell, and lungs. • Most IGF-1 is made in liver, also produced in many tissues. • IGF1R is similar to insulin receptor with intrinsic tyrosinekinase activity. • Insulin also can activate the type 1 IGF receptor but with affinity less than that of IGFs.
IGF transport protein • Circulating IGF-1 is associated with a family of proteins, IGF-binding proteins (IGFBPs), that serve as transport proteins and also mediate certain aspects of IGF-1 signaling. • Most IGF-1 in circulation is bound to IGFBP-3.
IGF-1 Preparations • Mecasermin:Recombinant human IGF-1 (rhIGF-I ) • (Increlex) • Mecaserminrinfabate(iPlex): Complex of rhIGF-I and rhIGFBP-3 (recombinant human insulin-like growth factor-binding protein-3) • Increases half-life. • iPlexhas been discontinued from marketing based on costs of manufacturing
Mecasermin • Bind to 1 IGF-1 receptors and stimulate multiple processes leading to staturalgrowth. • Administered to children with IGF-1 deficiency. • Children who unresponsive to GH therapy. • The most important toxicity is hypoglycemia. • Hypoglycemiaproduced by suppressing hepatic glucose production and stimulating peripheral glucose utilization • Hypoglycemia can be prevented by consumption of carbohydrate-containing meal before use. • Other side effects: Intracranial hypertension and asymptomatic elevation of liver enzymes.
GH Excess • Syndromes of excess secretion of GH typically are caused by somatotrope adenomas that oversecreteGH. • GH excess causes distinct clinical syndromes depending on age of the patient. • If the epiphyses are unfused, GH excess causes increased longitudinal growth, resulting in gigantism. • In adults, GH excess causes acromegaly
Pharmacotherapy of GH Excess: • Somatostatin Analogs: • Octreotide and Lanreotide • Growth Hormone Antagonists: • Pegvisomant
Somatostatin • Somatostatin, 14-amino-acid peptide is found in hypothalamus, other parts of central nervous system, pancreas, and other sites in GI tract. • Inhibits release of GH, TSH, glucagon, insulin, gastrin. • Has limited therapeutic usefulness because of its short duration of action. • Exogenous somatostatin is rapidly cleared from circulation, through kidney excretion.
Somatostatin Analogs • Two somatostatin analogs used: • Octreotideand lanreotide. • Regular octreotideadministered SC 2–4 times daily. • Slow-release formulation (IM) of octreotide andlanreotideadministered every 4 weeks.
Therapeutic Uses • Acromegaly • Carcinoid Tumor • Gastrinoma • Vasoactive Intestinal Peptide Tumor (VIPoma) • Pituitary Adenoma • Insulinoma • Glucagonoma • Esophageal varices, variceal bleeding • Diabetic Diarrhea Octreotide(50–200 mcg given sc, tds)
Lanreotide • Long-acting formulation of somatostatin analog. • Approved by FDA in 2007 for treatment of acromegaly. • Have effects comparable to those of octreotide on reducing GH levels and normalizing IGF-I concentrations.
Octreotide Side Effects • GI disturbances: Diarrhea, nausea, flatulence, steatorrhea • Gallbladder abnormalities: Gallstones, biliary sludge • Cardiac abnormalities: arrhythmias, sinus bradycardia • Hyperglycemia • Pain at the site of injection
Growth Hormone Antagonists • Pegvisomant
Growth Hormone Antagonists • Pegvisomant (SOMAVERT) is GH receptor antagonist that used for treatment of acromegaly. • Is polyethylene glycol (PEG) derivative of mutant GH. • Can cross-link GH receptors but incapable of inducing receptor activation. • Pegvisomant binds to GH receptor but does not activate JAK-STAT signaling or stimulate IGF-1 secretion. • Administered subcutaneously
Pegvisomant • Pegvisomant is highly effective alternative for use in acromegaly in patients who have not responded to SST analogs. • Should not be used in patients with an elevation of hepatic transaminases
Pharmacoherapy of Prolactin Excess
Prolactin • 198-amino-acid peptide hormone produced in the anterior pituitary. • Structure resembles of GH. • Prolactin, acting viaprolactin receptors • Milk production is stimulated by prolactin. • Plays important role in inducing growth and differentiation of the ductaland lobuloalveolarepithelium. • Prolactin hasno therapeutic uses
Prolactin • Deficiencyof prolactin occur in rarestates of pituitary deficiency or hypothalamic destruction. • Much more commonly, prolactin is elevated as a result of prolactin-secreting adenomas.
Hyperprolactinemia • Hyperprolactinemia is a relatively common endocrine abnormality that can result from : • Hypothalamic or pituitary diseases • Prolactinomas: microadenomasor macroadenomas. • Dopamine receptor antagonists: chlorpromazine, haloperidol, Metoclopramide, Reserpine • Presentation: • In women, causes galactorrhea, amenorrhea, infertility. • In men, causes loss of libido, erectile dysfunction, infertility.
Hyperprolactinemia • Diagnosis: MRI images • Medical therapy: Dopamine agonist is indicated in microprolactinomas for control of symptomatic galactorrhea, restoration of gonadal function, or when fertility is desired. • Alternatively, estrogen replacement may be indicated if fertility is not desired.
D2 receptor Agonist Dopamine is physiologic inhibitor of prolactinrelease. • D2 receptor Agonist: • Bromocriptine(Parlodel) • Cabergoline(Dostinex) • Pergolide(Perrmax) • Ergot derivatives • These agents (especially cabergoline)generally decrease both prolactin secretion and size of adenoma • Bromocriptine are also effective in inhibiting GH release (Acromegaly) and Parkinson's Disease. Pregnancy Category: B
















