Download
1 / 20
200 likes | 349 Views
CKD – 22% Medicare Costs More than CHF. 1. ESRD Costs 1992 – 2010 The cost of ESRD is on the Rise and continues to climb each year. 2. We do not serve our patients well!. Late stage CKD and ESRD patients are vulnerable and complex yet we do not intervene until the disease has progressed.

E N D
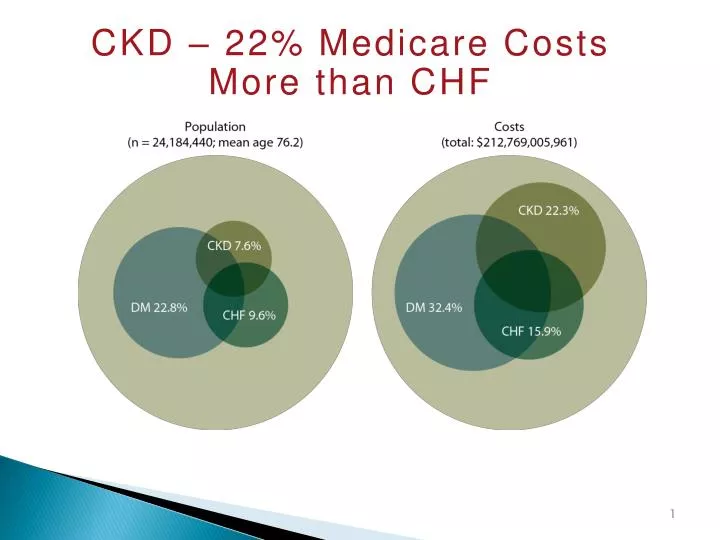
CKD – 22% Medicare Costs More than CHF 1
ESRD Costs 1992 – 2010 The cost of ESRD is on the Rise and continues to climb each year 2
We do not serve our patients well! • Late stage CKD and ESRD patients are vulnerable and complex yet we do not intervene until the disease has progressed. • ESRD patients have >3 co-morbidities, are prescribed 8-10medications, and consume 19 pills daily. • The mortality rate for ESRD patients on HD is seven times higher than the non-HD population. • ESRD patients are hospitalized on average,12 days/year. (Nissenson, 2012)
Renal ACOs: Are they in our future? • ESRD and CKD is an ideal disease state in which to pilot disease-specific ACOs. • Late stage CKD patients are clinically complex and care of these patients is disproportionately high. • ESRD consumes 7.5% of the Medicare budget or over $20 billion dollars. • ESRD encompasses 1.3% of the total Medicare population. (Centers for Medicare & Medicaid Services, 2010)
How can we use the ACO model to focus on disease prevention? • Creation of ACOs aim to decrease cost while improving patient outcomes. • Care of the Renal patient should be comprehensive and coordinated by an interdisciplinary team. This results in improved patients outcomes and expenditure savings. • Improved access to services affords the patient and the providers to manage disease states without acute episodes and worsening CKD.
What are healthcare providers looking to achieve within a Nephrology ACO? • Enhance effectiveness and efficiency of collaborative care to reduce fragmentation. • Improve coordination of care between healthcare providers and nurses. • Effective discharge planning and follow-up for renal patients. • Reduction in all-cause and cardiovascular hospitalizations. • Continued patient education with progression to self management of disease state. • Establishment of Advanced Care directives to avoid confusion in late disease stages.
Defining Expected Outcomes • Disease specific care needs to be based on appropriate healthcare utilization. • The Nephrology team needs to identify how the CKD and ESRD patient will utilize care and how often it will be required. • Reasonable use of healthcare services in order to meet expected goals will decrease more costly healthcare associated with care of the renal patient.
Your Nephrology team can improve utilization… • Implementation of evidence-based protocols. • Development of new care models. • Continued disease specific education. To provide quality cost effective care, stakeholders, providers, and team members must be flexible and willing to develop new care models designed to “push the limits”.
Embrace the concept now…Change is coming • The emergence and development of ACO models is occurring now! This represents what is likely to be a permanent shift in healthcare delivery and reimbursement. • Be aware of the emerging models and prepare for the change.
A local program has evolved… • In an attempt to improve patient outcomes for renal patients, NSLIJ invested in the creation of a CKD/ ESRD program. • This program was designed to follow patients with late stage CKD. • Through education and advocacy patients are better prepared to manage their disease state. • A long term goal is for the patient to effectively self manage their disease state.
What does this “program” do? • Aim to improve the coordination of care for CKD patients stage 3-5. • Improve outcomes and QOL for late stage CKD and ESRD. • Decrease fragmentation of care. • Provide supportive coordinated care to CKD patients in order to prepare the patient to effectively “self manage” their disease.
Program Goals • Care Managers are essential; they aim to better prepare the patient through education. • Focus is on medication reconciliation, home safety, overcoming barriers to follow up care, self management and recognition of worsening disease S/S, and identifying realistic health goals in order to decrease the poor pt. outcomes seen in CKD and ESRD.
Program Focus… • Early identification and management of CKD. We are currently working with and managing CKD 3-5. • Upon diagnosis, patients are referred to appropriate resources. Patient education and engagement begins. • Late stage focus shifts and education is primarily towards renal replacement therapy, fistula first goals, presentation and availability of home modalities (PD, cycler, and HD),preparation with advanced directives, and preventing hospital admissions.
The Triple Aim… • “Better Care, Lower Cost, Better Patient Experience” • The objective is to define how we can deliver on all three objectives. This requires a proactive, coordinated approach at prevention, early identification, and early intervention in the earlier stages. In the later stages care coordination w/ other subspecialty. This requires an infrastructure supported by care coordinators, navigators, and NPs to achieve the triple aim.
Achieving the goals… • The program uses a variety of patient interaction and monitoring techniques to meet program goals. • This is done through a combination of routine office visits, home visits, monthly telephone calls, telephonic weight management, and educational sessions.
What are patients and providers saying about this new program? Patient Feedback 85 year old woman: Patient reports, “problems with her kidneys”. Knowledge deficits. By end of visit says nurse “was a Godsend”. 24 year old creatinine > 10.0 reduced to engage on modality/access. Nurse met with patient, chose PD and catheter scheduled. The mother referred to the program as a “gift from God” 24 year old patient was schedule for home-based dialysis. All of his possessions were destroyed during Hurricane Sandy and there was nowhere to sit and administer self-dialysis. Nurse Practitioner worked through the American Kidney Fund (AKF) to receive a grant. This was utilized to purchase a new mattress. Physician Feedback “This the story of an elderly lady w/ diabetes and advanced kidney disease who was resistant to diuretic therapy, in part due to an allergic reaction to one type and side effects from another. She eventually became oxygen dependent because of fluid overload interfering w/ her breathing. The HT nurse, at the time of the home visit, found out the patient was on a very high Salt diet (while she was trying to eat healthily given the limitation of her diabetes and kidney disease). Based on CM instructions (a low Na diet), she lost almost 20 lbs of fluid. And she is now no longer requiring oxygen at home. Even more surprisingly her kidney function has remained stable. I am sure that if we would have done the same thing w/ high dose diuretics, her kidney function would have gotten worse, perhaps precipitating the need for dialysis”
Re-defining delivery of care • As new care models for the ESRD patient emerge, a paradigm shift to a more holistic approach must occur. • Team members must work to improve overall quality of life and decrease fragmentation of care. • YOU are in the unique position to advocate for change and work to actively improve outcomes for patients with CKD.
You can be an agent for change! • Programs should be designed to include case management, proactive intervention on admission and re-admission events, a multi-disciplinary care team, and patient education. • As we embark on this new era in Healthcare, you will have the opportunity to advocate for change and work to actively improve the lives of persons with CKD. The future of Nephrology is you!
Conclusion • CKD patients will undoubtedly benefit from a multidisciplinary team approach with basic tenants in education, prevention, and disease management. Organized, accountable care has the ability to make a difference in the lives of our patients. • An ESRD/CKD specific ACO would serve as an avenue to deliver high-quality, patient-centered care.
REFERENCES • American Hospital Association. (2010, December 1). American hospital association underpayment by Medicare and Medicaid fact sheet. Retrieved April 10, 2013, from http://www.aha.org/content/00-10/10medunderpayment.pdf • Cheung-Larivee, K. (2013, January 28). ACOs hone in on diseases. Retrieved March 15, 2013, from FierceHealthcare: http://www.fiercehealthcare.com/node/76131/print • Centers for Medicare and Medicaid Services. (2013, February 4). CMS announces new initiative to improve End- Stage Renal Disease care (ACO reading room). Retrieved March 10, 2013, from Davita- Accountable Kidney Care Collaborative: http://accountablekidneycare.com/files/ESRD-Announcement_PR-FINAL.PDF • Centers for Medicare and Medicaid Services. (2013, February 4). Comprehensive ESRD care model (ACO reading room). Retrieved March 12, 2013, from Davita- Accountable Kidney Care Collaborative: http://accountablekidneycare.com/files/ESRD-CMS_Fact_Sheet-FINAL.pdf • Costs of ESRD. (2012) (Chapter 11). Retrieved March 25, 2013, from United States Renal Data System: http://www.usrds.org/2012/view/v2_11.aspx • International comparisons. (2012) (Chapter 12). Retrieved March 25, 2013, from United States Renal Data System: http://www.usrds.org/2012/view/v2_12.aspx • Nissenson, A. (2012, July 1). Renal ACO: A model for care coordination. Accountable Care News, 3(7). Retrieved April 1, 2013, from www.AccountableCareNews.com. • Nissenson, A., Maddux, F. W., Velez, R., Mayne, T., & Parks, J. (2012). Accountable care organizations and ESRD: The time has come. American Journal of Kidney Disease, 59(5), 724-733. • Renal Physicians Association. (2012, December 3). RPA guidance on Nephrologist Interactions with accountable care organizations (ACO reading room). Retrieved March 1, 2013, from Davita- Accountable Kidney Care Collaborative: http://accountablekidneycare.com/files/2012_RPA_Guidance_on_Nephrologist-ACO_Interactions_12-03-2012_FINAL.pdf • Robinson, J. (2011). Hospitals respond to Medicare payment shortfalls by both shifting costs and cutting them, based on market concentration. Health Affairs, 30(7), 1265-1271. • US Department of Health and Human Services.2020 Topics and objectives - Chronic kidney disease. (2013, March 28) (Chronic kidney disease-Healthy people). Retrieved April 1, 2013, from US Department of Health and Human Services: http://www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicId=6 • US Department of Health and Human Services.Chronic kidney disease. (2012, September 6) (Chronic kidney disease- Healthy people). Retrieved April 1, 2013, from US Department of Health and Human Services: http://www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicId=6 • United States Renal Data System. (2012). Healthy people 2020 (ESRD Healthy people 2020). Retrieved March 25, 2013, from USRDS: http://www.usrds.org/2012/view/v2_00hp.aspx • Weiss, J. (2013). ACOs are here to stay. Retrieved March 15, 2013, from Davita: http://accountablekidneycare.com/files/october-2012-physician-update-ACOs-are-here-to-stay.pdf • Williams, A., Nesse, R., & Wood, D. (2012). Delivering accountable care to patients with complicated chronic illness: How does it fit into care models and do Nephrologists have a role? American Journal of Kidney Disease, 59(5), 601-603.