Download
1 / 2
20 likes | 131 Views
Diagnostic Tip: Where are the P waves? What do you do when you perform a lead II rhythm strip on a dog or cat and you don't see any P waves? The answer depends on the clinical history, the heart rate and the regularity of the R-R intervals.

E N D
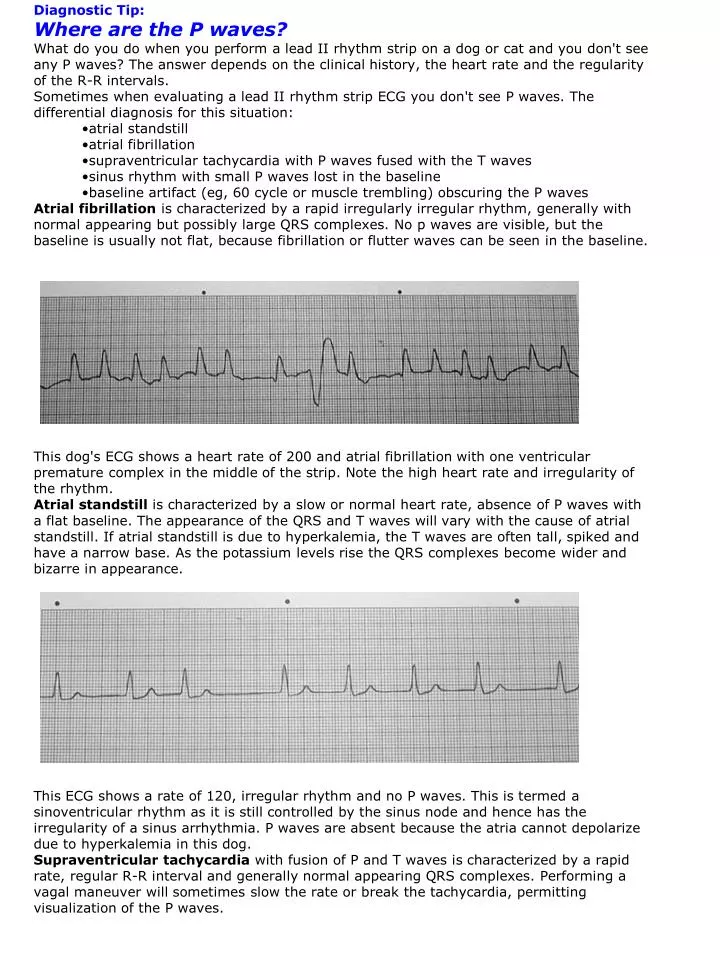
Diagnostic Tip: Where are the P waves? • What do you do when you perform a lead II rhythm strip on a dog or cat and you don't see any P waves? The answer depends on the clinical history, the heart rate and the regularity of the R-R intervals. • Sometimes when evaluating a lead II rhythm strip ECG you don't see P waves. The differential diagnosis for this situation: • atrial standstill • atrial fibrillation • supraventricular tachycardia with P waves fused with the T waves • sinus rhythm with small P waves lost in the baseline • baseline artifact (eg, 60 cycle or muscle trembling) obscuring the P waves • Atrial fibrillation is characterized by a rapid irregularly irregular rhythm, generally with normal appearing but possibly large QRS complexes. No p waves are visible, but the baseline is usually not flat, because fibrillation or flutter waves can be seen in the baseline. • This dog's ECG shows a heart rate of 200 and atrial fibrillation with one ventricular premature complex in the middle of the strip. Note the high heart rate and irregularity of the rhythm. • Atrial standstill is characterized by a slow or normal heart rate, absence of P waves with a flat baseline. The appearance of the QRS and T waves will vary with the cause of atrial standstill. If atrial standstill is due to hyperkalemia, the T waves are often tall, spiked and have a narrow base. As the potassium levels rise the QRS complexes become wider and bizarre in appearance. • This ECG shows a rate of 120, irregular rhythm and no P waves. This is termed a sinoventricular rhythm as it is still controlled by the sinus node and hence has the irregularity of a sinus arrhythmia. P waves are absent because the atria cannot depolarize due to hyperkalemia in this dog. • Supraventricular tachycardia with fusion of P and T waves is characterized by a rapid rate, regular R-R interval and generally normal appearing QRS complexes. Performing a vagal maneuver will sometimes slow the rate or break the tachycardia, permitting visualization of the P waves.
This dog's ECG shows a heart rate of 300, regular R-R interval and no P waves. The very high heart rate causes the P and T wave to fuse, so a distinct P wave is not evident. • P waves are sometimes difficult to see in patients with a rapid ventricular tachycardia. However, as the sinus node and atria are activated at a different rate than the ventricles in animals with ventricular tachycardia, P waves can usually be identified moving in and out of the QRS complexes. • In patients with a normal heart rate, normal appearing QRS complexes, and absence of P waves on the rhythm strip, you have to consider the possibility of a sinus rhythm with P waves being small and lost in the baseline. If you suspect that P waves may be present, hat can you do to try to make this diagnosis? The following techniques will often allow you to visualize P waves when they don't appear on the lead II rhythm strip: • Repeat an ECG obtaining all 6 limb leads (I, II, III, aVR, aVL, aVF). Sometimes the P waves are isoelectric in lead II, but will be visible in one of the other limb leads. • If P waves aren't visible on any of the limb leads and the QRS complexes are small, increase the sensitivity setting on the ECG machine to make everything larger. • If P waves are still not visible, run a chest lead. The chest lead typically makes the complexes larger. To run a chest lead place the exploring lead (5th lead) on the chest over the left apex of the heart. If your ECG machine does not have a 5th lead wire, move the lead from the left hind leg to the left chest wall and run the ECG on lead II. • If P waves are still not visible and the rate is slow, you can administer atropine at 0.04 mg/kg (0.02 mg/lb) IM and repeat the ECG 20-30 minutes later. Depending on the cause of the bradycardia the atropine will speed up the heart rate and often makes the P waves larger. • SummaryWhen you can't see P waves, the first step is to eliminate baseline artifact and then evaluate multiple leads and sensitivities to make sure that small P waves aren't lurking in the baseline. Once you are convinced that P waves don't exist, you are probably dealing with either atrial fibrillation (rapid irregularly irregular rhythm), supraventricular tachycardia (rapid regular rhythm), or atrial standstill (slow regular or irregular rhythm).