Download
1 / 22
220 likes | 531 Views
Myocardial Perfusion SPECT Should NOT Be Routine in Symptomatic Patients with Excellent Exercise Capacity. V. Froelicher, MD Professor of Medicine Stanford University VA Palo Alto HCS. Myocardial Perfusion SPECT Should NOT Be Routine in Symptomatic Patients with Excellent Exercise Capacity

E N D
Myocardial Perfusion SPECT Should NOT Be Routine in Symptomatic Patients with Excellent Exercise Capacity V. Froelicher, MD Professor of Medicine Stanford University VA Palo Alto HCS
Myocardial Perfusion SPECT Should NOT Be Routine in Symptomatic Patients with Excellent Exercise Capacity • For simplicity sake let us avoid the philosophical issues regarding this: • no test should be routine for all patients • clinical judgment and the art of medicine (incldg patients own desires and needs) should be foremost in the decision to test or not to test. • Quality of life issues: “are you able to do everything you want to do?”
Myocardial Perfusion SPECT Should NOT Be Routine in Symptomatic Patients with Excellent Exercise Capacity • Assumptions: • Symptoms equal chest pain • Exercise capacity obtained from an exercise test. • Excellent exercise capacity => 10 METs
What are the Questions being asked? • Are these symptoms due to Coronary Disease? • Do these symptoms put this patient at high risk for a Cardiac Event? • Is a invasive intervention appropriate? • If due to CAD, what is the culprit lesion? • Does the baseline ECG invalidate ST analysis?
Regarding 2 of the Questions: • If due to CAD, what is the culprit lesion? • ST depression does not localize, ST elevation does but rare … Then yes, SPECT needed • Does the baseline ECG invalidate ST analysis? • More than one mm ST depression, LBBB, WPW, IVCD, paced rhythm …. Then yes, SPECT is needed
The other Questions • Are these symptoms due to Coronary Disease? • If no resting ECG abnormalities and scores used the exercise ECG sufficient … then No, SPECT not needed • Do these symptoms put this patient at high risk for a Cardiac Event? • DTS and other prognostic scores sufficient … then No, SPECT not needed • Is an invasive intervention appropriate?
Males Choose only one per group <40=low prob 40-60= intermediate probability >60=high probability
Kaplan-Meier Survival curves for the “all-comers” prognostic score. METs equally important to clinical variables SCORE = (1=yes, 0=no) METs<5 + Age>65 + History of CHF + History of MI or Q wave a=0, b=1, c=2, d=more than 2
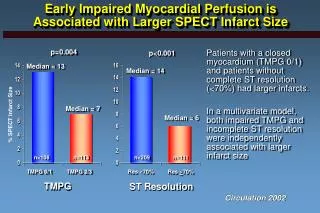
Most pertinent: Snader CE, Marwick TH, Pashkow FJ, Harvey SA, Thomas JD, Lauer MS.JACC 1997;30(3):641-8 Cleveland Clinic: Importance of estimated functional capacity as a predictor of all-cause mortality among patients referred for exercise perfusion: 3,400 patients CONCLUSIONS: In this clinically low risk group, estimated functional capacity was a strong and overwhelmingly important independent predictor of all-cause mortality among patients undergoing exercise Tl-201 SPECT testing.
Next Most pertinent:McCully RB, Roger VL, Mahoney DW, Burger KN, Click RL, Seward JB, Pellikka PA. J Am Coll Cardiol 2002 Apr 17;39(8):1345-52 Outcome after abnormal exercise echo for patients with good exercise capacity. Methods: 1,874 patients with CAD who had good exercise capacity but abnormal exercise ECHOs; cardiac events (cardiac death or nonfatal MI). CONCLUSIONS: ECHO descriptors of the extent and severity of exercise-related LV dysfunction were of independent and incremental prognostic value. Stratification of patients into low- and higher risk subgroups was possible.
Ventilatory (VO2) • Cardiac Output x a-v O2 Difference • VE x (% Inspired Air Oxygen Content - Expired Air Oxygen Content) • External Work Performed
What is a MET? • Metabolic Equivalent Term • 1 MET = "Basal" aerobic oxygen consumption to stay alive = 3.5 ml O2 /Kg/min • By convention just divide ml O2/Kg/min by 3.5
Key MET Values (part 1) • 1 MET = "Basal" = 3.5 ml O2 /Kg/min • 2 METs = 2 mph on level • 4 METs = 4 mph on level • < 5METs = Poor prognosis if < 65; • limit immediate post MI; • cost of basic activities of daily living
Key MET Values (part 2) • 10 METs = As good a prognosis with medical therapy as CABS • 13 METs = Excellent prognosis, regardless of other exercise responses • 16 METs = Aerobic master athlete • 20 METs = Aerobic athlete
Importance of METs • 10 to 15% increase in survival per MET • Can be increased by 25% by a training program
Cause of change in Practice? • Not reimbursement but obvious superiority or impression of superiority of other testing • “The Doctor does the test he gets paid (the most) for” … the Doctor’s Dilemma, GB Shaw, 1926 • Are we getting our monies worth???
Medicare Costs and Savings(response to drop in TM reimbursement from $350 to $150)