Download
1 / 25
250 likes | 525 Views
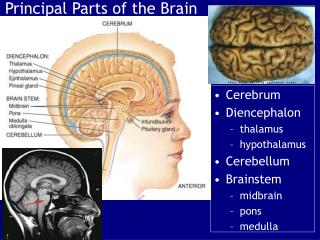
Biological Bases of Behaviour. Lecture 11: Brain Damage. Kalat (2001) p133. Learning Outcomes. By the end of this lecture you should be able to: 1 . Describe the major causes of brain damage. 2 . Explain the processes involved in recovery from neural damage. . 1. Vascular Disorders.

E N D
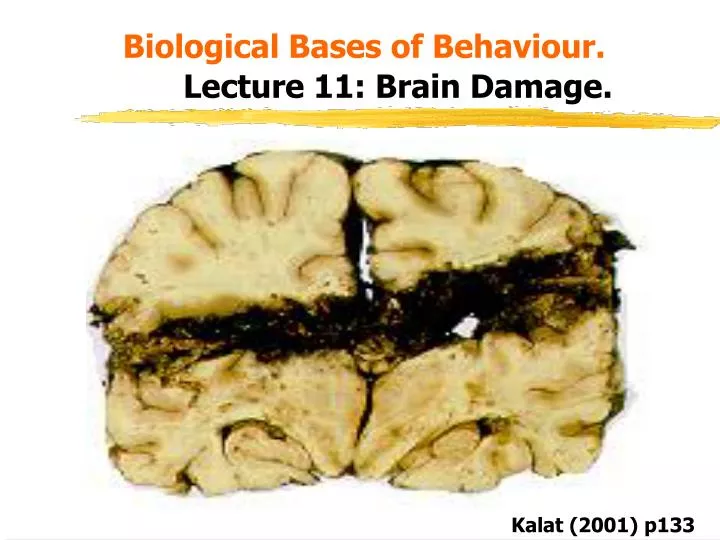
Biological Bases of Behaviour.Lecture 11: Brain Damage. Kalat (2001) p133
Learning Outcomes. • By the end of this lecture you should be able to: • 1. Describe the major causes of brain damage. • 2. Explain the processes involved in recovery from neural damage.
1. Vascular Disorders. • CNS cells are easily damaged, especially when their blood supply is impaired. • Disruption of neural blood supply by disease or accident is called a stroke. • These are very common with an incidence of around 2 per 1000. • 35% of stroke sufferers die within a year, the remainder experience varying degrees of impairment depending upon the brain regions affected. Kolb & Whishaw (1990) p 132
Strokes (continued). • The most common cause of strokes is blockage of the artery (ischemia) caused by the build up of fat, less common is the rupture of an artery (haemorrhage). • Both types produce the same effect. • A stroke produces an area of dead tissue (infarct), the size of which depends on where the damage occurred. • The behavioural symptoms depends upon the exact location of the damage, e.g. a lesion in the visual cortex can produce an area of blindness, one affecting the hippocampus can affect memory.
Migraine. • A migraine headache is a transient ischemia, and they affect around 5-20% of the population. • They consist of visual disturbances, headache, movement difficulties, and aphasia, the precise symptoms depending on the areas affected. There are 2 main types: • i) Classic migraine: Experienced by 12% of sufferers and includes a visual aura due to constriction of one or more cerebral arteries. This may be followed by a severe headache, which may last hours or days. • ii) Common migraine: Occurs in 80% of sufferers, with no visual aura but feelings of nausea. This is followed by a cluster headache in the head or face lasting about 2 hours. • These are more common in younger people and can be triggered by anxiety, fatigue, bright lights, food allergies, and hormonal changes during the menstrual cycle.
2. Traumatic Head Injuries. • Cerebral trauma is the commonest form of brain damage in young people (vehicle/horse-riding/industrial accidents, warfare). Such trauma can affect the brain in several ways: • Direct damage to the brain in which neurons are damaged directly. • Disruption of blood supply resulting in ischemia and possibly infarction. • Bleeding within the skull, leading to increased intracranial pressure. • Bruising of the brain leading to swelling. • A compound fracture of the skull can open the brain to infection. • Scarring of brain tissue can later become a focus for epileptic seizures.
Types of Head Injury • i) Open-Head Injuries. • The skull is penetrated, or fragments of bone penetrate the brain. • Victims remain conscious and have distinctive symptoms that may undergo rapid and spontaneous recovery. • The specificity of neurological symptoms following open-head injuries makes these patients especially good research subjects. E.g. Phineas Gage described by Macmillan (1984).
ii) Closed Head Injuries. • These result from a blow to the head : • The damage at the site of the blow is called a coup as the brain is compacted by the bone being forced inward. • The pressure on the brain at the time of the coup forces the brain against the opposite side of the skull, producing a countercoup. • Movement of the brain causes twisting and shearing of nerve fibres, producing tiny lesions in frontal and temporal lobes. Such damage also affects fibres in the corpus callosum and anterior commissure producing a disconnection syndrome. • The bruises and strains may produce bleeding within the skull which forms a growing mass (haematoma) exerting pressure on surrounding structures.
Impairments Following A Closed-Head Injury. • CHI’s are accompanied by loss of consciousness (coma) resulting from strain on fibres in the reticular formation. • Coma duration serves as a predictive measure of the severity of the damage, it correlates directly with subsequent mortality, intellectual impairment, and deficits in social skills. • Two kinds of impairments are seen following closed-head injuries. • Discrete impairments: Specific impairment of functions at the site of the coup or countercoup. Personality changes, aggression, and the inability to plan and organise are commonly seen. • Generalised Impairments: Less specific impairments resulting from diffuse cortical damage. Loss of mental speed and concentration problems are common.
3. Epilepsy. • This is characterised by recurrent excessive synchronised production of action potentials from many neurons, mainly due to decreased release of the inhibitory neurotransmitter GABA (During et al., 1995). • Such seizures are very common with 1 in 20 experiencing at least one fit in their lifetime, but multiple seizures are much rarer at 1 in 200. • The cause of epilepsy remained unknown until the invention of the electroencephalograph (EEG), which demonstrated that different types of epilepsy were associated with different abnormal electrical rhythms in the brain.
Characteristics of Epilepsy. • Sometimes epileptic seizures are symptomatic i.e. they can be linked with specific factors such as trauma, infection, drugs, or fever. • Other seizures are idiopathic, they arise spontaneously in the absence of other neurological disorders. Three common symptoms are often reported: • i) An aura, or warning of the impending seizure in the form of as odours or noises. • ii) Loss of consciousness which may consist of a complete collapse, or simply a 'staring into space', there is often amnesia of the seizure. • iii) Uncontrolled movements such as shaking and vocal utterances.
Classifications of Epilepsy. • a) Focal seizures: Begin locally and spread, they generally affect cortical motor areas so that an attack begins with jerks in the fingers, and then spreads so that the whole hand, and arm becomes affected. • b) Complex partial seizures: Originate in the medial temporal lobe and are characterised by the intrusion of repetitive thoughts, hallucinations, déjà vu, repetitive movements such as lip smacking, and a frozen posture. • c) Generalised seizures: In a Petit Mal seizure there is a loss of awareness during which there is motor activity such as blinking or rolling the eyes but the episodes are brief and seldom exceed 10 seconds.
Generalised Seizures continued. • In a Grand Mal seizure, the individual experiences an aura followed by loss of consciousness in which they stiffen, shake, and perhaps make noises, this is followed by post-seizure confusion and amnesia. Before the seizure Seizure onset Clonic phase Coma phase Kolb & Whishaw (1990) p 140
4. Tumours. • A tumour (neoplasm) is a mass of new tissue that persists and grows independently of its surrounding structures. • Some are unlikely to reoccur after removal (benign) but others are likely to regrow again (malignant), they are equally dangerous depending on their location. • There are several types distinguished on the basis of where they originate: • a) Glioma's: These arise from glial cells and infiltrate brain tissue. 45% of all brain tumours are of this type and they can be benign or malignant, there are three types: • i) Astrocytomas: Develop from the astrocytes, they are slow growing and commonest in adults over the age of 30. They are not often malignant, and can be easily treated.
Glioma’s continued. • iii) Glioblastomas: • These are highly malignant, rapidly growing, and are common in men over 35. They are difficult to treat and have poor life expectancy. • iii) Medulloblastomas: These are highly malignant and are found exclusively in the cerebellum of children, prognosis is very poor. glioblastoma Kolb & Whishaw (1990) p 145
b) Meningiomas Meningioma • These are growths attached to the meninges and so grow outside the brain. • They exert pressure on brain tissue. • As they do not enter the brain they can be removed easily. • They are generally benign. Kolb & Whishaw (1990) p 144
Recovery After Brain Damage. • Neurons cannot be replaced once destroyed or damaged. • However, some recovery often occurs following brain damage. How does this recovery take place? • It was assumed that another region of the brain took over the impaired functioning of a damaged region, but this only occurs in a limited manner. • E.g if motor cortex in the left hemisphere is damaged, the corresponding area of the right hemisphere takes over some function of the ipsilateral limbs but only by strengthening already existing ipsilateral pathways. • Much of the recovery seen following brain damage is achieved by the person making better use of unimpaired abilities or by learning to use abilities that appeared to be lost but were actually just impaired. • There are several factors in recovery:
1. Role of Stimulants. • Impairment following brain damage does not just reflect localised damage but also the 'knock-on' effects of that damage. • When a neuron dies, other neurons that depended upon that neuron for input also become impaired - this is called diaschisis. • Sutton et al., (1989) showed that injecting the stimulant amphetamine led to a significant improvement in undamaged neuron functioning following brain damage to adjacent regions. • Injections of antagonists such as haloperidol impaired behavioural recovery.
2. Axon Regrowth. • Damaged axons can regrow to a limited extent. For example damaged neurons in the peripheral nervous system grow back at around 1mm per day. • If a myelinated axon is severed the regenerating axons follows the myelin path back to its original target. • Sensory nerves find their way back to sensory receptors, and motor nerves to motor receptors, however they can sometimes re-connect to the wrong receptor. Kalat (2001) p138
3. Sprouting. • After axons have been damaged, cells that formerly received their synaptic input begin to secrete neurotrophins which induce nearby axons to form new branches (sprouts) that connect to the vacant synapses. Normal Loss of axon Sprouting Kalat (2001) p138
4. Heightened Sensitivity. • If a postsynaptic cell is deprived of input for a long time it becomes more sensitive to its neurotransmitter by creating additional receptors or by increasing their sensitivity. • This is known as denervation supersensitivity.
5. Cortical Reorganisation. • Following amputation, cortical reorganisation can occur; if a cortical area no longer receives input, other regions 'spread'. • Merzenich et al., (1984) showed that following amputation of a single finger, the area of somatosensory cortex previously sensitive to input from that finger became responsive to the other fingers and parts of the palm. Kalat (2001) p141
Phantom Limbs. • Many people who have lost a limb still perceive it vividly, these phantom limbs are very real to amputees even to the extent that they feel pain in their missing fingers. • Cortical areas representing the arms and face lie close together, if an arm is missing then the area of cortex previously responsive to the limb becomes responsive to the face. • Stroking the face will trigger sensations in the missing limb. • As the areas representing the feet and genitals also lie close together people, with amputated feet can feel their missing appendages during sexual stimulation as the representation of the genitals has spread into the now unused area representing the feet (Ramachandran & Herstein, 1998).
Influence of Age. • Neurons are gradually lost throughout life so that by age 60 dendrites have shrunk, many cells have been lost, and the sprouting process has slowed down. • These natural processes can exacerbate the effects of brain damage, such that recovery from brain damage in the elderly is always much less than in the young. • Recovery in the very young may be dramatic, for example if a child under the age of 2 loses their entire left hemisphere they may develop near-normal speech. • However the young brain is more sensitive, and damage to certain developing neurons may lead to severe problems in later life (autism, perhaps schizophrenia).
References and Bibliography. • Kalat, J.W. (1995). Biological Psychology. • Kolb, B., & Whishaw, I.Q. (1990). Fundamentals of Human Neuropsychology. • Macmillan, M.B. (1986). A wonderful journey through skull and brains: the travels of Mr. Gage's tamping iron. Brain and Cognition, 5: 67-107. • Merzenich, M.M., Nelson, R.J., Stryker, M.P., Cynader, M.S., Schoppman, A., Zook, J.M. (1984). Somatosensory cortical map changes following digit amputation in adult monkeys. Journal of Comparative Neurology, 224: 591-605. • Sutton, R.L., Hovda, D.A., & Feeney, D.M. (1989). Amphetamine accelerates recovery of locomotor function following bilateral frontal cortex ablation in rats. Behavioural Neuroscience, 103: 837-841.