Download
1 / 1
10 likes | 145 Views
Establishment and validation of a standard protocol for the detection of minimal residual disease in B lineage childhood acute lymphoblastic leukaemia by flow cytometry in a multi-centre setting; a report from the UK ALL Flow MRD group.

E N D
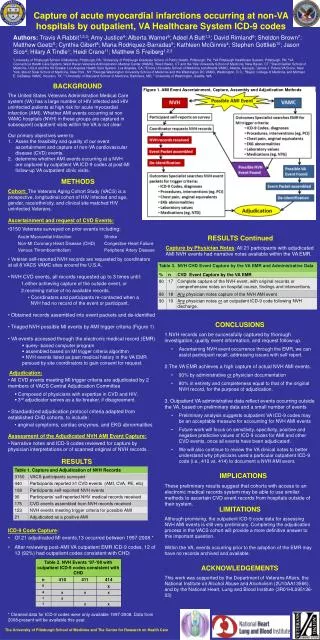
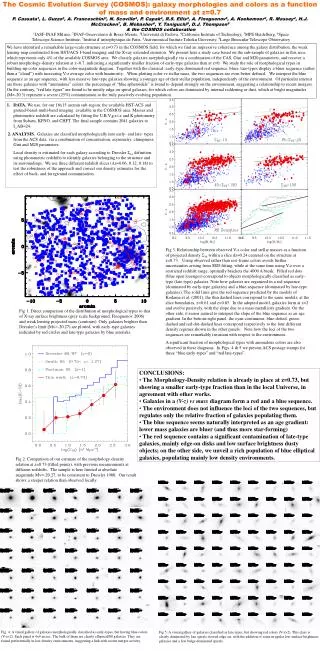
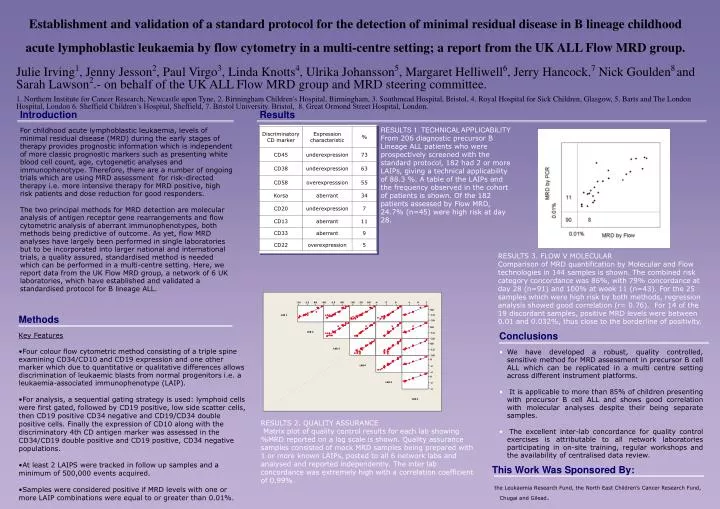
Establishment and validation of a standard protocol for the detection of minimal residual disease in B lineage childhood acute lymphoblastic leukaemia by flow cytometry in a multi-centre setting; a report from the UK ALL Flow MRD group. Julie Irving1, Jenny Jesson2, Paul Virgo3, Linda Knotts4, Ulrika Johansson5, Margaret Helliwell6, Jerry Hancock,7 Nick Goulden8and Sarah Lawson2.- on behalf of the UK ALL Flow MRD group and MRD steering committee. 1. Northern Institute for Cancer Research, Newcastle upon Tyne, 2. Birmingham Children's Hospital, Birmingham, 3. Southmead Hospital, Bristol, 4. Royal Hospital for Sick Children, Glasgow, 5. Barts and The London Hospital, London 6. Sheffield Children’s Hospital, Sheffield, 7. Bristol University. Bristol, 8. Great Ormond Street Hospital, London. Introduction For childhood acute lymphoblastic leukaemia, levels of minimal residual disease (MRD) during the early stages of therapy provides prognostic information which is independent of more classic prognostic markers such as presenting white blood cell count, age, cytogenetic analyses and immunophenotype. Therefore, there are a number of ongoing trials which are using MRD assessment for risk-directed therapy i.e. more intensive therapy for MRD positive, high risk patients and dose reduction for good responders. The two principal methods for MRD detection are molecular analysis of antigen receptor gene rearrangements and flow cytometric analysis of aberrant immunophenotypes, both methods being predictive of outcome. As yet, flow MRD analyses have largely been performed in single laboratories but to be incorporated into larger national and international trials, a quality assured, standardised method is needed which can be performed in a multi-centre setting. Here, we report data from the UK Flow MRD group, a network of 6 UK laboratories, which have established and validated a standardised protocol for B lineage ALL. Results RESULTS 1. TECHNICAL APPLICABILITY From 206 diagnostic precursor B Lineage ALL patients who were prospectively screened with the standard protocol, 182 had 2 or more LAIPs, giving a technical applicability of 88.3 %. A table of the LAIPs and the frequency observed in the cohort of patients is shown. Of the 182 patients assessed by Flow MRD, 24.7% (n=45) were high risk at day 28. RESULTS 3. FLOW V MOLECULAR Comparison of MRD quantification by Molecular and Flow technologies in 144 samples is shown. The combined risk category concordance was 86%, with 79% concordance at day 28 (n=91) and 100% at week 11 (n=43). For the 25 samples which were high risk by both methods, regression analysis showed good correlation (r= 0.76). For 14 of the 19 discordant samples, positive MRD levels were between 0.01 and 0.032%, thus close to the borderline of positivity. • Methods • Key Features • Four colour flow cytometric method consisting of a triple spine examining CD34/CD10 and CD19 expression and one other marker which due to quantitative or qualitative differences allows discrimination of leukaemic blasts from normal progenitors i.e. a leukaemia-associated immunophenotype (LAIP). • For analysis, a sequential gating strategy is used: lymphoid cells were first gated, followed by CD19 positive, low side scatter cells, then CD19 positive CD34 negative and CD19/CD34 double positive cells. Finally the expression of CD10 along with the discriminatory 4th CD antigen marker was assessed in the CD34/CD19 double positive and CD19 positive, CD34 negative populations. • At least 2 LAIPS were tracked in follow up samples and a minimum of 500,000 events acquired. • Samples were considered positive if MRD levels with one or more LAIP combinations were equal to or greater than 0.01%. • Conclusions • We have developed a robust, quality controlled, sensitive method for MRD assessment in precursor B cell ALL which can be replicated in a multi centre setting across different instrument platforms. • It is applicable to more than 85% of children presenting with precursor B cell ALL and shows good correlation with molecular analyses despite their being separate samples. • The excellent inter-lab concordance for quality control exercises is attributable to all network laboratories participating in on-site training, regular workshops and the availability of centralised data review. RESULTS 2. QUALITY ASSURANCE Matrix plot of quality control results for each lab showing %MRD reported on a log scale is shown. Quality assurance samples consisted of mock MRD samples being prepared with 1 or more known LAIPs, posted to all 6 network labs and analysed and reported independently. The inter lab concordance was extremely high with a correlation coefficient of 0.99%. This Work Was Sponsored By: the Leukaemia Research Fund, the North East Children’s Cancer Research Fund, Chugai and Gilead.