Download
1 / 10
120 likes | 651 Views
EKG Interpretation: Hypertrophy and Enlargement of the Heart. Humayun J. Chaudhry, DO, MS, FACP, FACOI Chairman, Department of Medicine N.Y. College of Osteopathic Medicine of NYIT October 31, 2002. Lecture Goals and Objectives.

E N D
EKG Interpretation: Hypertrophy and Enlargement of the Heart Humayun J. Chaudhry, DO, MS, FACP, FACOI Chairman, Department of Medicine N.Y. College of Osteopathic Medicine of NYIT October 31, 2002
Lecture Goals and Objectives • Understand how to recognize and analyze, using criteria or typical findings, enlargement of the heart on an EKG • Be able to recognize the EKG patterns associated with atrial and ventricular hypertrophy • Be aware of important pearls in the EKG analysis of hypertrophy • Relax, proceed slowly and methodically
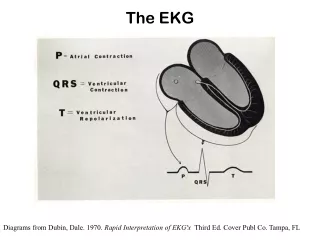
Introduction • Myocardial hypertrophy means an increase in the thickness (muscle mass) of the walls of the atria or ventricles • Dilatation, or enlargement, is an increase in the internal diameter of the atria or ventricles • EKG manifestations of hypertrophy and dilatation may be similar • R Ventricle lies anterior to L Ventricle • L Ventricle is 3-4X mass of R Ventricle and depolarization of LV produces the majority of the QRS deflection
Introduction • Hypertrophy is caused by a pressure overload, in which the heart is forced to pump blood against an increased resistance • Dilatation/Enlargement is typically caused by a volume overload, as in certain valvular diseases • Nomenclature • Atrial Enlargement (aka Atrial Abnormalities) • Ventricular Hypertrophy
Left Atrial Enlargement • EKG Findings • Broad, notched, P wave (greater than 0.10 sec in duration) in Leads I, II, aVL • Large terminal negative P wave deflection (greater than 0.04 sec) in V1, representing depolarization forces traveling posteriorly in larger L atrium • Also known as “P mitrale” because of the mitral valve diseases (mitral stenosis, mitral regurgitation) associated with it
Right Atrial Enlargement • EKG Findings • Tall, peaked P wave (greater than 2.5 mm in height in Leads II, III, aVF • Large initial positive P wave deflection in Lead V1 • Duration of P wave usually normal (less than 0.10 sec) • Also known in literature as “P pulmonale” or “P congenitale” because of the pulmonary or congenital heart conditions, respectively, that are associated with this entity
Left Ventricular Hypertrophy (LVH) • EKG Criteria (Know This!) • Increased voltage of QRS complexes (most important criteria) • R in V5 or V6 plus S in V1 > 35 mm • R in V5 or V6 > 26 mm (Memorize**) • R in aVL > 11 mm • R in I plus S in III > 25 mm • Depressed ST segment and inverted T in Leads V5, V6 (and I, aVL) • Increased duration of QRS complex. Why? • Left Axis Deviation (LAD) • Estes/Estes-Romhilt Criteria
Right Ventricular Hypertrophy (RVH) • EKG Criteria (diagnosis can be difficult,) • Right Axis Deviation (RAD) – Memorize** • Increased QRS complex voltage • R/S ratio in V1 > 1, or • R in V1 plus S in V5 orV6 = or > 10.5 mm, or • R in V1 > 7 mm, or • R in aVR > 5 mm, or • S in V1 < 2 mm, or • Prominent S in V5, V6 • Repolarization changes (ST-T) in V1, V2 • Mild increase in QRS duration • Small Q in V1
Hypertrophy EKG Pearls • For the advanced student: • Q waves in V1, V2, and V3 may be seen in LVH and may be mistaken for an old anterior myocardial infarction • RVH may be masked by complete RBBB • In RVH, chest leads show a reversal of usual QRS chest pattern with tall R in V1, V2 and deep S in V5, V6