Download
1 / 1
10 likes | 85 Views
ROBOTIC PROSTHESIS AND ITS BENEFITS Jennifer Rodriguez and Elliot Felipe The E piscopal Cathedral School . ABSTRACT.

E N D
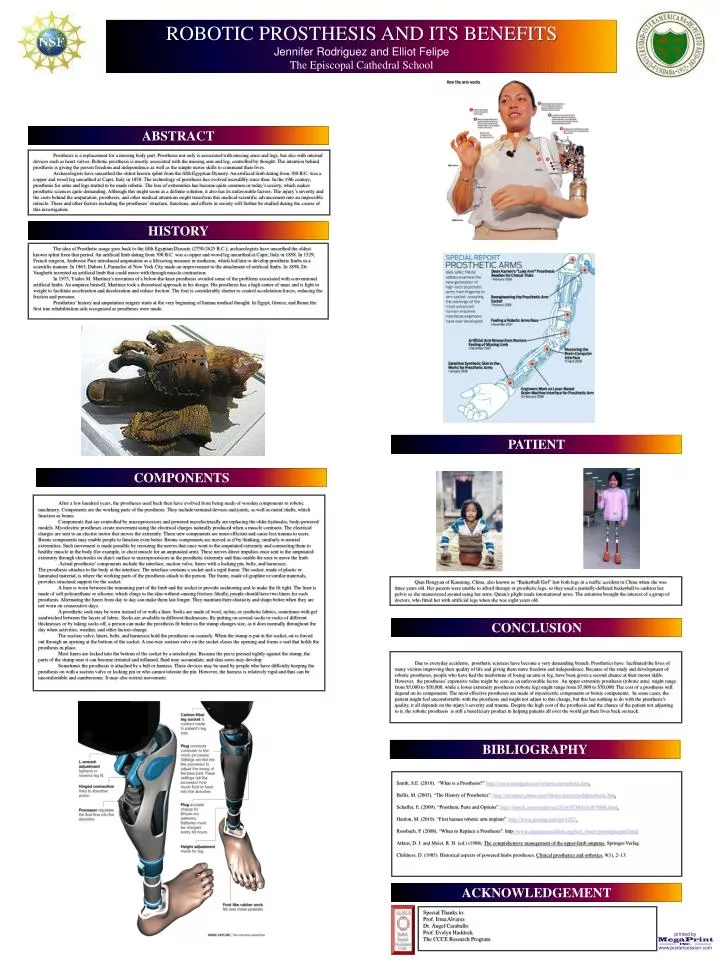
ROBOTIC PROSTHESIS AND ITS BENEFITS Jennifer Rodriguez and Elliot Felipe The Episcopal Cathedral School ABSTRACT Prosthesis is a replacement for a missing body part. Prosthesis not only is associated with missing arms and legs, but also with internal devices such as heart valves. Robotic prosthesis is mostly associated with the missing arm and leg, controlled by thought. The intention behind prosthesis is giving the person freedom and independence as well as the simple motor skills to command their lives. Archaeologists have unearthed the oldest known splint from the fifth Egyptian Dynasty. An artificial limb dating from 300 B.C. was a copper and wood leg unearthed at Capri, Italy in 1858. The technology of prosthesis has evolved incredibly since then. In the 19th century, prosthesis for arms and legs started to be made robotic. The loss of extremities has become quite common in today’s society, which makes prosthetic sciences quite demanding. Although this might seem as a definite solution, it also has its unfavorable factors. The injury’s severity and the costs behind the amputation, prosthesis, and other medical attentions might transform this medical-scientific advancement into an impossible miracle. These and other factors including the prostheses’ structure, functions, and effects in society will further be studied during the course of this investigation. HISTORY The idea of Prosthetic usage goes back to the fifth Egyptian Dynasty (2750-2625 B.C.); archaeologists have unearthed the oldest known splint from that period. An artificial limb dating from 300 B.C. was a copper and wood leg unearthed at Capri, Italy in 1858. In 1529, French surgeon, Ambroise Pare introduced amputation as a lifesaving measure in medicine, which led him to develop prosthetic limbs in a scientific manner. In 1863, Dubois L Parmelee of New York City made an improvement to the attachment of artificial limbs. In 1898, Dr. Vanghetti invented an artificial limb that could move with through muscle contraction. In 1975, Ysidro M. Martinez's invention of a below-the-knee prosthesis avoided some of the problems associated with conventional artificial limbs. An amputee himself, Martinez took a theoretical approach in his design. His prosthesis has a high center of mass and is light in weight to facilitate acceleration and deceleration and reduce friction. The foot is considerably shorter to control acceleration forces, reducing the friction and pressure. Prosthetics’ history and amputation surgery starts at the very beginning of human medical thought. In Egypt, Greece, and Rome the first true rehabilitation aids recognized as prostheses were made. PATIENT COMPONENTS After a few hundred years, the prostheses used back then have evolved from being made of wooden components to robotic machinery. Components are the working parts of the prosthesis. They include terminal devices and joints, as well as metal shafts, which function as bones. Components that are controlled by microprocessors and powered myoelectrically are replacing the older hydraulic, body-powered models. Myoelectric prostheses create movement using the electrical charges naturally produced when a muscle contracts. The electrical charges are sent to an electric motor that moves the extremity. These new components are more efficient and cause less trauma to users. Bionic components may enable people to function even better. Bionic components are moved as if by thinking, similarly to natural extremities. Such movement is made possible by rerouting the nerves that once went to the amputated extremity and connecting them to healthy muscle in the body (for example, to chest muscle for an amputated arm). These nerves direct impulses once sent to the amputated extremity through electrodes on skin's surface to microprocessors in the prosthetic extremity and thus enable the user to move the limb. Actual prostheses’ components include the interface, suction valve, liners with a locking pin, belts, and harnesses. The prosthesis attaches to the body at the interface. The interface contains a socket and a rigid frame. The socket, made of plastic or laminated material, is where the working parts of the prosthesis attach to the person. The frame, made of graphite or similar materials, provides structural support for the socket. A liner is worn between the remaining part of the limb and the socket to provide cushioning and to make the fit tight. The liner is made of soft polyurethane or silicone, which clings to the skin without causing friction. Ideally, people should have two liners for each prosthesis. Alternating the liners from day to day can make them last longer. They maintain their elasticity and shape better when they are not worn on consecutive days. A prosthetic sock may be worn instead of or with a liner. Socks are made of wool, nylon, or synthetic fabrics, sometimes with gel sandwiched between the layers of fabric. Socks are available in different thicknesses. By putting on several socks or socks of different thicknesses or by taking socks off, a person can make the prosthesis fit better as the stump changes size, as it does normally throughout the day when activities, weather, and other factors change. The suction valve, liners, belts, and harnesses hold the prosthesis on securely. When the stump is put in the socket, air is forced out through an opening at the bottom of the socket. A one-way suction valve on the socket closes the opening and forms a seal that holds the prosthesis in place. Most liners are locked into the bottom of the socket by a notched pin. Because the pin is pressed tightly against the stump, the parts of the stump near it can become irritated and inflamed, fluid may accumulate, and skin sores may develop. Sometimes the prosthesis is attached by a belt or harness. These devices may be used by people who have difficulty keeping the prosthesis on with a suction valve or locking pin or who cannot tolerate the pin. However, the harness is relatively rigid and thus can be uncomfortable and cumbersome. It may also restrict movement. Qian Hongyan of Kunming, China, also known as “Basketball Girl” lost both legs in a traffic accident in China when she was three years old. Her parents were unable to afford therapy or prosthetic legs, so they used a partially-deflated basketball to cushion her pelvis as she maneuvered around using her arms. Quian’s plight made international news. The attention brought the interest of a group of doctors, who fitted her with artificial legs when she was eight years old. CONCLUSION Due to everyday accidents, prosthetic sciences have become a very demanding branch. Prosthetics have facilitated the lives of many victims improving their quality of life and giving them more freedom and independence. Because of the study and development of robotic prostheses, people who have had the misfortune of losing an arm or leg, have been given a second chance at their motor skills. However, the prostheses’ expensive value might be seen as an unfavorable factor. An upper extremity prosthesis (robotic arm) might range from $5,000 to $50,000, while a lower extremity prosthesis (robotic leg) might range from $7,000 to $70,000. The cost of a prosthesis will depend on its components. The most effective prostheses are made of myoelectric components or bionic components. In some cases, the patient might feel uncomfortable with the prosthesis and might not adjust to this change, but this has nothing to do with the prosthesis's quality, it all depends on the injury’s severity and trauma. Despite the high cost of the prosthesis and the chance of the patient not adjusting to it, the robotic prosthesis is still a beneficiary product in helping patients all over the world get their lives back on track. BIBLIOGRAPHY Smith, S.E. (2010). “What is a Prosthesis?”.http://www.wisegeek.com/what-is-a-prosthesis.htm. Bellis, M. (2003). “The History of Prosthetics”. http://inventors.about.com/library/inventors/blprosthetic.htm. Schaffer, E. (2009). “Prosthetic Parts and Options”. http://merck.com/mmhe/sec25/ch307888/ch307888b.html. Hanlon, M. (2010). “First human robotic arm implant”. http://www.gizmag.com/go/4282/. Rossbach, P. (2008). “When to Replace a Prosthesis". http://www.amputee-coalition.org/fact_sheets/prosreplacprof.html. Atkins, D. J. and Meier, R. H. (ed.) (1988). The comprehensive management of the upper-limb amputee. Springer-Verlag. Childress, D. (1985). Historical aspects of powered limbs prostheses. Clinical prosthetics and orthotics, 9(1), 2–13. ACKNOWLEDGEMENT SpecialThanksto: Prof. Irma Alvarez Dr. ÁngelCaraballo Prof. Evelyn Haddock The CCCE Research Program