Download
1 / 23
230 likes | 652 Views
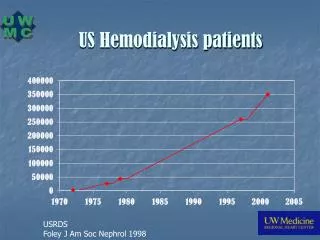
Hemodialysis and Hemofiltration in Pediatrics: An Approach to Intoxication. Karen Papez MD University of Michigan Pediatric Nephrology, Dialysis & Transplantation 3rd annual PCRRT, Orlando, FL . 2002 Annual Report of American Association of Poison Control Centers.

E N D
Hemodialysis and Hemofiltration in Pediatrics: An Approach to Intoxication Karen Papez MD University of Michigan Pediatric Nephrology, Dialysis & Transplantation 3rd annual PCRRT, Orlando, FL
2002 Annual Report of American Association of Poison Control Centers • Nearly 2.4 million human exposures reported by 64 participating poison centers in 2002. • 4.9% increase from 2001 • Children <3 yrs: 39% of all human exposures • Children <6 yrs: 51.6% of all exposures *Pediatricians and pediatric subspecialists need to be prepared to handle the majority of poison exposures. • Watson WA et al. Am J Emerg Med 21: 2003 • Litovitz TL et al. Am J Emerg Med 20: 2002
Enhanced Elimination Techniques for Poisonings • Enhanced elimination techniques were used for 1457 cases (0.06%) in 2002. • A near 8% increase over 2001 reports • Hemodialysis: 1400 [up 9% from 2001] • Hemoperfusion: 30 [down 33% from 2001] • Other Extracorporeal Procedures: 27 *Pediatric nephrologists and intensivists need to be equipped with advanced techniques to handle such clinical situations.
Treatment Measures Availablefor Poisonings • Enhance Elimination (Cont.) • Extracorporeal Methods • Hemodialysis • Standard • High Efficiency/High Flux • Hemofiltration • Hemoperfusion • Exchange Transfusion • Plasma exchange
Toxin Clearance • What effects clearance? • Volume of distribution • Whether or not the drug is primarily renally excreted (competing pathways) • Protein binding • Molecular size of the drug • Mode of therapy-HD, CVVH vs CVVHD vs CVVHDF • Hemofilter membrane properties Pond, SM - Med J Australia 1991; 154: 617-622
HEMODIALYSIS • Optimal drug characteristics for removal: • Relative molecular mass < 500 Daltons • Water soluble • Small Vd (< 1 L/Kg) • Minimal plasma protein binding • Single compartment kinetics • Low endogenous clearance (< 4ml/Kg/min) Pond, SM - Med J Australia 1991; 154: 617-622
HEMOFILTRATION • Optimal drug characteristics for removal: • Relative molecular mass less than the cut-off of the filter fibres (usually < 40,000 daltons) • Small Vd (< 1 L/Kg) • Single compartment kinetics • Low endogenous clearance (< 4ml/Kg/min) Pond, SM - Med J Australia 1991; 154: 617-622
Additional Factors when Considering Enhanced Elimination Methods • Drug kinetics should be reviewed • Note: Kinetics may differ in an overdose situation • Valproic acid: 90% protein bound with nl levels • Valproic acid: 70% bound at levels of 135 mcg/ml : 35% bound at levels of 300 mcg/ml *The higher the levels and the more unbound drug that exists, the more effectively it may be removed.
Case 1 • 14 year old female with history of depression, found slurring words, intermittently confused in her bedroom. • During period of lucency, told mother she drank something a schoolmate gave her to “get high.” States this was 18 hours before presentation to local ER.
Physical Exam at Admission to PICU • T 38.8 P 125 RR 32 BP 158/75 Wt 75 Kg • Generally: GCS variable, from verbal response to voice to mild response to pain. • HEENT: Pupils equally round, sluggishly reactive to light, mucous membranes dry • Resp: Deep, tachypneic, clear to auscultation • CV: RRR, no murmur, peripheral pulses 2/4 • Abd: Soft, nondistended, hypoactive bowel sounds
148 121 13 98 5.4 7 2.1 9.4 38 0.3 4.8 4.0 59 143 11.7 16.8 163 50.4 7.24 / 18 / 113 / 8 UA SG 1.015, pH 5, normal for all substrates AG 20 Calc osm 306 Serum osm 311 CPK 388 NH3 38 Ethanol negative Urine drug screen negative βhCG negative Salicylate <1 Acetaminophen <10 Ethylene glycol 24.2 Laboratory Analyses
Calculated Osmolality with Dialysis in Ethylene Glycol Intoxication HD Started CVVHDF Started CT-190 Prisma dialyzer Multiflo-100 BFR -HD 250 ml/min -CVVHDF 180 ml/min PO4 based dialysate - 4L/1.73m2/hr
Case 2 • 12 year old female with history of bipolar disorder had started an increased dose of lithium 6 weeks prior to admission. • Was slurring her speech on morning of admission, and had irregular constant movements of her arms and legs.
Physical Exam at Admission to PICU • T afebrile P 82 RR 23 BP 104/46 Wt 33 Kg • Generally: Confused, slurring speech • HEENT: NC, AT, Mucous membranes moist • Resp: Clear to auscultation • CV: Regular rate and rhythm, no murmur • Abdomen: Soft, normoactive bowel sounds • Skin: Erythematous rash over abdomen • Neuro: Athetoid movements as noted in HPI
133 107 31 73 4.3 22 1.2 6.8 7.0 35 0.6 4.1 25 215 10.5 12.1 176 34.4 7.36 / 50 / 28 / 28 UA SG 1.010, pH 6.5, pro 1+, ket 2+, LE 1+, otherwise normal AG 4 CPK 939 NH3 38 Ethanol and volatile acids negative Urine drug screen negative βhCG negative Salicylate <1 Acetaminophen <10 Lithium 7.34 EKG First degree heart block, PR 188 ms, prolonged QTc 520 ms Laboratory Analyses
Lithium Clearance on Dialysis HD Started CVVHD Started CVVHD Stopped CT-190 Prisma dialyzer Multiflo-100 BFR -HD 250 ml/min -CVVHDF 180 ml/min PO4 based dialysate - 4L/1.73m2/hr
Lithium Redistributes from Intracellular Compartment: Arrows indicate beginning and end of HD. A significant rebound in serum concentration occurred after a 5-hr HD treatment with recurrence of neurologic impairment. An additional 4-hour hemodialysis treatment was then begun. From Goldfarb DS in Goldfrank’s Toxologic Emergencies, 7th Ed. 2002 Hemofiltration May Attenuate Rebound Phenomenon!
CVVHD Following HD for Lithium Poisoning Li Therapeutic range 0.5-1.5 mEq/L HD started CT-190 (HD) Prisma dialyzer -Multiflo-60 (#1,2) -Multiflo-100 (#3) BFR- HD -pt # 1 200 ml/min -pt # 2 325 ml/min -pt # 3 250 ml/min BFR- CVVHD 200 ml/min - All 3 pts. PO4 Based dialysate at 2L/1.73m2/hr (#1,2) 4L/1.73m2/hr (#3) CVVHD started
Conclusions • High efficiency hemodialysis and hemofiltration may alter the current “treatment of choice”. • Pediatric nephrologists need to be aware that more than one treatment option exists for many toxicology situations, and the modality selected should be that tailored to their patient’s needs.
ACKNOWLEDGEMENTS • THERESA MOTTES • TIM KUDELKA • BETSY ADAMS • TAMMY KELLY • ROBIN NIEVAARD • DAVID KERSHAW • PATRICK BROPHY
OTHER ISSUES • Optimal prescription • Biocompatible filters - may increase protein adsorption • Maximal blood flow rates (i.e. good access) • Physiological solution (ARF vs non ARF) • Potential removal of antidote • Counter-current dialysate maximal removal of toxins
Specific Antidotes Should be used adjunctively with supportive therapy. Examples: • N-acetyl cysteine [for Acetaminophen] • Benzodiazepines [for Flumazenil] • Flumazenil [for Benzodiazepines] • Naloxone [for Opiates] • Calcium [for Calcium channel blockers] • Atropine [for Acetylcholinesterase inhibitors] • Fomepizole [for Ethylene glycol, Methanol, & Diethylene Glycol] • Ethanol [for Ethylene glycol, Methanol, & Diethylene Glycol]