Download
1 / 25
320 likes | 502 Views
Spinal Anesthesia. A Seminar by : Stephanie N. Ammari. Regional Anesthesia. Is the use of local anesthetics to block sensations of pain from a large area of the body , such as ; an arm or leg or the abdomen … based on the dermatomes .

E N D
Spinal Anesthesia A Seminar by : Stephanie N. Ammari
Regional Anesthesia • Is the use of local anesthetics to block sensations of pain from a large area of the body , such as ; an arm or leg or the abdomen … based on the dermatomes . • Neuraxial Anesthesia refers to local anesthetics placed around the nerves of the CNS , such as ; spinal anesthesia , epidural anesthesia , caudal anesthesia .
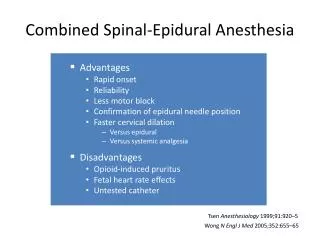
THE ROLE OF NEURAXIAl ANESTHESIA IN ANESTHETIC PRACTICE • Neuraxial blocks may reduce the incidence of venous thrombosis and pulmonary embolism, cardiac complications inhigh-risk patients, bleeding and transfusion requirements, vascular graft occlusion, and pneumonia and respiratory depression following upper abdominal or thoracic surgery in patients with chronic lung disease. • neuraxial blocks are routinely employedfor labor analgesia, cesarian delivery, orthopedic surgery, perioperative analgesia, and chronic pain management.
THE ROLE OF NEURAXIAl ANESTHESIA IN ANESTHETIC PRACTICE • The Sick Elderly Patient . A spinal anesthetic withlittle orno intravenous sedation may reduce thelikelihood of postoperative delirium or cognitive dysfunction, which is sometimes seen in the elderly. • The Obstetric Patient . Is associated with less maternal morbidityand mortality than is general anesthesia.
Mechanism of Action • Theprincipal site of action for neuraxial blockade isbelieved tobe the nerve root, at least during initial onset of block. • Local anestheticisinjected into : CSF … (spinal anesthesia) the epidural space … (epidural and caudal anesthesia)
Manifestations • Cardiovascular Manifestations … produce variable decreasesin blood pressure that may be accompanied bya decreasein heart rate. • Pulmonary Manifestations …there is only a smalldecrease in vital capacity, which results from a lossof the abdominal muscles’ contribution to forced expiration. • Gastrointestinal Manifestations … Neuraxialblock–induced sympathectomy allows vagal “dominance” with a small, contractedgut and activeperistalsis.
Indications • lower abdomen . • Perineum . • Hip. • Lower extremities . • Lower spine . *** for example : Hernia , gynaecology & obstetrics procedures (e.g : cesarian delivery ) , surgical procedure on lower limbs . *Upper abdominal procedures (eg,gastrectomy) have been performed with spinal or epidural anesthesia, butbecause it can be difficult to safely achievea sensory level adequatefor patient comfort thesetechniques are less commonly used.
Contraindications to neuraxial blockade. • Absolute • Infection at the site ofinjection. • Lack of consent . • Coagulopathy or otherbleeding diathesis. • Severe hypovolemia. • Increased intracranial pressure .
Contraindications to neuraxial blockade. • Relative 1. Sepsis . 2. Uncooperative patient . 3. Preexistingneurological deficits . 4. Demyelinatinglesions . 5. Stenoticvalvularheartlesions . 6. Left ventricular outflowobstruction(hypertrophic obstructive cardiomyopathy). 7. Severe spinaldeformity .
Contraindications to neuraxial blockade. • Controversial • Prior back surgery at the site of injection . • Complicated surgery. • Prolonged operation. • Major blood loss Maneuvers that compromiserespiration .
Anatomy • The laminae extend between the transverse processes andthe spinous processes, and the pedicle extends between the vertebral bodyand thetransverse processes • Thepedicles are notched superiorly andinferiorly, these notches forming the intervertebral foramina from which spinal nerves exit . • Ventrally, the vertebral bodies and intervertebral disks are connected andsupported by the anterior and posterior longitudinal ligaments . Dorsally, the ligamentumflavum, interspinousligament, and supraspinous ligament provide additional stability. Usingthe midline approach, a needle passes through thesethree dorsal ligaments and through an oval space between the bony lamina and spinous processes of adjacent vertebra.
The spinal cord normally extends from theforamen magnum tothe level of L1 in adults . Inchildren, the spinal cord ends at L3 and moves up with age. • The spinal canal contains the spinal cord with its coverings (the meninges), fatty tissue, anda venous plexus . The meninges are composed of three layers: the pia mater, thearachnoid mater, and thedura mater. • Cerebrospinal fluid (CSF) is containedbetween thepia and arachnoid maters in the subarachnoid space.
Surface Anatomy Spinous processes are usuallypalpable and help to define the midline. Ultrasound can be used when landmarks are not palpable . With the arms at the side, the spinous process of T7 is usually at the same level as the inferior angle of the scapulae . (Tuffier’s line) usually crosses either thebody of L4or the L4–L5 interspace.
Patient Positioning • Sitting Position .
Anatomic approach A . Midline Approach . B. Paramedian Approach . C. Assessing Level of Blockade With knowledge ofthe sensory dermatomes , the extent of sensory block can be assessed by a blunted needle or a piece of ice. D . Ultrasound-Guided Neuraxial Blockade . ultrasound guidance can facilitate neuraxial blockade in patients with poorly palpable landmarks.
Factors affecting the dermatomalspread of spinal anesthesia. • Most important factors : 1. Baricity of anesthetic solution . 2. Position of the patient # During injection # Immediately after injection . 3. Drug dosage . 4. Siteof injection .
Factors affecting the dermatomal spread of spinal anesthesia. • Other factors : • Age . • Cerebrospinal fluid • Curvature of the spine . • Drug volume . • Intraabdominalpressure. • Needle direction. • Patient height. • Pregnancy.
Baricity of the local anesthetic • Baricity : Local anesthatic density relative to CSF . • A hyperbaric solution of local anesthetic is denser (heavier) than CSF … solution migrates caudally when the patient is in the sitting position . • A hypobaricsolution is less dense (lighter) than CSF . • An isobaric solution :its density = CSF density… solution tends to remain atthe level of injection. • *** The best type to be used is the HYPERBARIC solution. • *** to change a hypobaric solution into hyperbaric … use DEXTROSE
Spinal Anesthetic Agents The best agent is the Bupivacaine