Download
1 / 1
10 likes | 235 Views
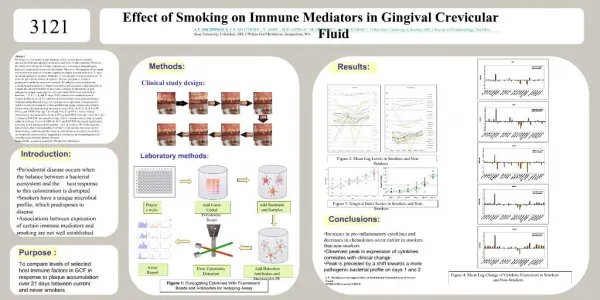
Distribution of Systemic Macrolides to Gingival Crevicular Fluid. WEITING HO 1 AND J.D. WALTERS 1. 1 The Ohio State University , College of Dentistry , Section of Periodontology, Columbus, OH.

E N D
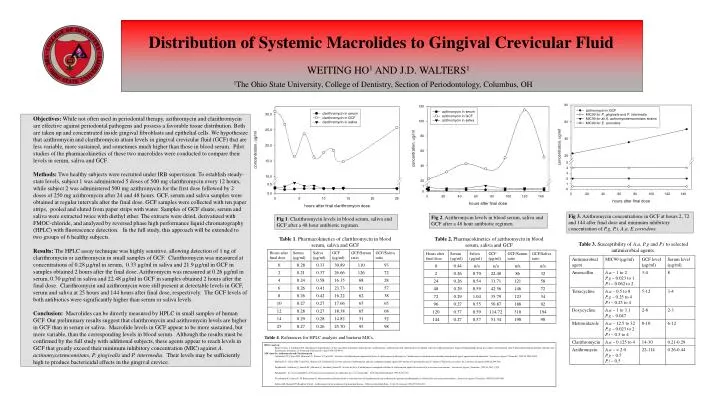
Distribution of Systemic Macrolides to Gingival Crevicular Fluid WEITING HO1 AND J.D. WALTERS1 1The Ohio State University, College of Dentistry, Section of Periodontology, Columbus, OH • Objectives: While not often used in periodontal therapy, azithromycin and clarithromycin are effective against periodontal pathogens and possess a favorable tissue distribution. Both are taken up and concentrated inside gingival fibroblasts and epithelial cells. We hypothesize that azithromycin and clarithromycin attain levels in gingival crevicular fluid (GCF) that are less variable, more sustained, and sometimes much higher than those in blood serum. Pilot studies of the pharmacokinetics of these two macrolides were conducted to compare their levels in serum, saliva and GCF. • Methods: Two healthy subjects were recruited under IRB supervision. To establish steady-state levels, subject 1 was administered 5 doses of 500 mg clarithromycin every 12 hours, while subject 2 was administered 500 mg azithromycin for the first dose followed by 2 doses of 250 mg azithromycin after 24 and 48 hours. GCF, serum and saliva samples were obtained at regular intervals after the final dose. GCF samples were collected with ten paper strips, pooled and eluted from paper strips with water. Samples of GCF eluate, serum and saliva were extracted twice with diethyl ether. The extracts were dried, derivatized with FMOC-chloride, and analyzed by reversed phase high performance liquid chromatography (HPLC) with fluorescence detection. In the full study, this approach will be extended to two groups of 6 healthy subjects. • Results: The HPLC assay technique was highly sensitive, allowing detection of 1 ng of clarithromycin or azithromycin in small samples of GCF. Clarithromycin was measured at concentrations of 0.28 µg/ml in serum, 0.33 µg/ml in saliva and 21.9 µg/ml in GCF in samples obtained 2 hours after the final dose. Azithromycin was measured at 0.26 µg/ml in serum, 0.70 µg/ml in saliva and 22.48 µg/ml in GCF in samples obtained 2 hours after the final dose. Clarithromycin and azithromycin were still present at detectable levels in GCF, serum and saliva at 25 hours and 144 hours after final dose, respectively. The GCF levels of both antibiotics were significantly higher than serum or saliva levels. • Conclusion: Macrolides can be directly measured by HPLC in small samples of human GCF. Our preliminary results suggest that clarithromycin and azithromycin levels are higher in GCF than in serum or saliva. Macrolide levels in GCF appear to be more sustained, but more variable, than the corresponding levels in blood serum. Although the results must be confirmed by the full study with additional subjects, these agents appear to reach levels in GCF that greatly exceed their minimum inhibitory concentration (MIC) against A. actinomycetemcomitans, P. gingivalis and P. intermedia. Their levels may be sufficiently high to produce bactericidal effects in the gingival crevice. Fig 3.Azithromycin concentrations in GCF at hours 2, 72 and 144 after final dose and minimum inhibitory concentration of P.g, P.i, A.a, E.corrodens. Fig 2. Azithromycin levels in blood serum, saliva and GCF after a 48 hour antibiotic regimen. Fig 1. Clarithromycin levels in blood serum, saliva and GCF after a 48 hour antibiotic regimen. Table 1. Pharmacokinetics of clarithromycin in blood serum, saliva and GCF Table 2. Pharmacokinetics of azithromycin in blood serum, saliva and GCF Table 3. Susceptibility of A.a, P.g and P.i to selected antimicrobial agents. Table 4. References for HPLC analysis and bacteria MICs. • HPLC analysis • Sastre Torano J, Guchelaar HJ. Quantitative determination of the macrolide antibiotics erythromycin, roxithromycin, azithromycin and clarithromycin in human serum by high-performance liquid chromatography using pre-column derivatization with 9-fluorenylmethyloxycarbonyl chloride and fluorescence detection. J Chromatogr B Biomed Sci Appl 1998;720:89-97. • MIC data for Azithromycin and Clarithromycin • Goldstein EJC, Citron DM, Merriam CV, Warren Y, Tyrrell K. Activities of telithromycin compared to those of erythromycin, azithromycin, clarithromycin, roxithromycin and other antimicrobial agents against unusual anaerobes. Antimicrob Agents Chemother 1999;43:2801-2805. • Merriam CV, Citron DM, Tyrrell KL, Warren YA, Goldstein EJ. In vitro activity of azithromycin and nine comparator agents against 296 strains of oral anaerobes and 31 strains of Eikenella corrodens. Int J Antimicrob Agents 2006;28:244-248. • Pajukanta R, Asikainen S, Saarela M, Alaluusua S, Jousimies-Somer H. In vitro activity of azithromycin compared with that of erythromycin against Actinobacillus actinomycetemcomitans. Antimicrob Agents Chemother 1992;36:1241-1243. • Pajukanta R. In vitro susceptibility of Porphyromonas gingivalis to azithromycin, a novel macrolide. Oral Microbiol Immunol 1993;8:325-326. • Piccolomini R, Catamo G, Di Bonaventura G. Bacteriostatic and bactericidal in vitro activities of clarithromycin and erythromycin against periodontopathic Actinobacillus actinomycetemcomitans. Antimicrob Agents Chemother 1998;42:3000-3001 • Sefton AM, Maskell JP, Beighton D et al. Azithromycin in the treatment of periodontal disease. Effect on microbial flora. J Clin Periodontol 1996;23:998-1003.