Download
1 / 36
370 likes | 701 Views
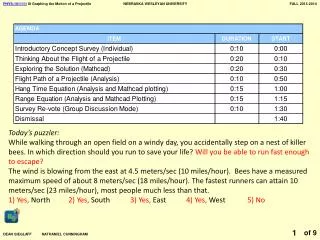
Pediatric Puzzler. August 2007. Chief Complaint. “My baby is not right and she’s got yellow eyes”. HPI. 5 week old Caucasian female who presents with lethargy, jaundice and poor weight gain. PCP referred to a gastroenterologist for rising direct hyperbilirubinemia. PMH. Birth history:

E N D
Pediatric Puzzler August 2007
Chief Complaint • “My baby is not right and she’s got yellow eyes”
HPI • 5 week old Caucasian female who presents with lethargy, jaundice and poor weight gain. • PCP referred to a gastroenterologist for rising direct hyperbilirubinemia
PMH • Birth history: • FT C/S for failure to progress • BW 3.61 kg • NICU for 6 days b/c of hypothermia and hypoglycemia sepsis w/u done was negative • NICU labs: • initial glucose 27 • bili t/d (6dol) 15.3/1 • Diet: Breastfed until DOL 8 when changed to hydrolyzed protein formula secondary to persistent elevated bili. Feeding well per mom • Elimination: 10 wet diapers/day, 2 yellow-brown seedy stools/day
The next PCP visit • Patient was seen by PCP for jaundice at 5 weeks. • She was noted to have a bili t/d of 9.5/4.5 • Patient was referred to a gastroenterologist for further workup
Definition of the Day • What is direct hyperbilirubinemia exactly? • Direct bilirubin >2 mg/dL • Direct bilirubin > 20% of total bili • Direct hyperbilirubinemia effects 1 in 2500 infants. • That’s fairly common! • BUT…it’s never normal!
Do you have any questions? Don’t be afraid to ask…
Physical Exam • Wt 3.55 kg (10-25%) Lt 55 cm (75%) HC 39 cm (50%) • T 98.7 P 160 R 36 B/P 92/58 • Gen: quiet, responds to mom, no apparent distress, minimal subcutaneous fat, no dysmorphic features • HEENT: mm dry, sclera icteric, OP clear • CV/RESP: RRR no murmurs, CTAB • Abd: soft, ND, no HSM, no masses • GU: normal female • Skin: capillary hemangioma in right axilla • Neuro: grossly intact, + moro, +suck, +grasp
What do you think? Top 3 diagnoses Top 3 tests …with rationale por favor
What Labs Do I Get? • Elevated LFTs • Hepatocellular injury • Elevated Alkphos and GGT-- point to obstructive conditions • Make sure to fractionate the bili! • TORCH titers, Ucx, Sweat test, Urine reducing substances if indicated by Hx/PE • Follow up on NBS! • Consider liver function studies as well.
Labs • 139 106 13 101 4.6 18 0.7 10.3 • Alb 2.3 • Bili t/d 8.9/4.2 • AST 50/ALT 22/ AP 385 • ESR 8 (0-20) • NBS- normal from the state lab • 14.6 11 537 33 s 14 l 81 m3 • Ammonia 58 (29-70) • α 1 antitrypsin - normal • UA- 1.004 pH 5; 1 WBC; 0 RBC; no RS • Cultures sent BCx, UCx, CSF Cx
While in the hospital… • IVF • IV Antibiotics • Breastfeed or formula ad lib • Is and Os monitored • Scans ordered
Scan on, scan on… • Abdominal u/s • Reason for order: Exclude surgical cause of extrahepaticbiliary obstruction • Result: NORMAL • Hepatobiliary nuclear scan • Reason for order: Look for patency of biliary tract R/O biliaryatresia • Result: NORMAL, gallbladder visualized and excretion was normal
On Rounds • The astute T3, just joking it’s a L3, questions the UOP on rounds. She noticed that it was 6 cc/kg/hr. • The resident had failed to check the baby’s Is & Os for the day. Whoops.
Hmm… mo’ problems As a group, refine your problem definition and differential Do we need any other labs/ tests? Why?
Causes of Direct Hyperbilirubinemia • IntrahepaticCholestasis • Primary • Alagille Syndrome • Idiopathic Neonatal Hepatitis • Acquired • Drugs/ Fetal Alcohol • Sepsis • TORCH • Hep B • HIV • TPN • Endocrine Disorders • Hypothyroidism • Hypopituitarism • ExtrahepaticCholestasis • BiliaryAtresia • Choledochal cyst • Choledocholithiasis cyst • Genetic/ Metabolic • α 1 antitrypsin • Cystic fibrosis • Galactosemia/ Fructosemia • Gaucher disease • Niemann Pick • Glycogen storage disease • Trisomy 18 • Trisomy 21 • Tyrosinemia
Alagille Syndrome AD genetic d/o with paucity of bile ducts. May also have PPS and vertebral defects Features: Long nose with bulbous tip Triangular face Broad forehead
Biliary Atresia • Most common and serious cause of direct hyperbilirubinemia • Destroys the intra- and extrahepaticbiliary tree • May also see acholic stools • Should be diagnosed before 2 months--- HIDA • Tx: Kasai then transplant
Other Causes of Conjugated Hyperbili • Idiopathic neonatal hepatitis • Self limited- resolves in 3-4 weeks • Giant cells are seen on biopsy • Alpha 1 Antitrypsin • Most common genetic cause of acute and chronic liver disease in children • Liver retains abnormally folded protein • May also develop lung disease (later in life)
Complications of Cholestasis • Coagulopathy • Fat malabsorption • Ascites • Encephalopathy
Back to Our Patient • What do we think about UOP of 6 cc/kg/hr? • What could be the cause? • Looking back at labs done during the hospitalization, it was noted that the serum sodium peaked at 149 mEq/L • What are we worried about now?
Diabetes Insipidus • “Flavorless Urine” • Characterized by: • Inability to concentrate urine • Polyuria • Polydipsia • Cause • ADH deficiency- Central • Lack of end organ response to ADH- Nephrogenic • Thick limb of ascending loop of Henle • Collecting duct
Diabetes Insipidus • Characteristics in infancy • FTT • Vomiting • Constipation • Unexplained fevers • Shock (hypovolemic) • Convulsions
More tests done… • Urine Osmolality= 167 mOsml/L (>200) • Serum Osmolality= 300 mOsml/L (275-295) • DDAVP was given UOsm of 310 mOsml/L • What type of Diabetes Insipidus is this? • CENTRAL • The kidney responded appropriately to DDAVP dose.
Don't Get Confused! DI SIADH • High serum Na • Low urine SG <1005 • Low urine osm 50-200 • Low vasopressin • Tx: DDAVP • Low serum Na • Low serum Cl • Inappropriately concentrated urine • Euvolemic or hypervolemic • Tx: Fluid restrict
What to do now? Why does this girl have central DI? What tests do we want now?
Correct! Get a MRI! • MRI was done- Pituitary was completely normal! • In Central DI- the signal on T1 is usually abnormal (not as bright (hyperintense) as usual) • Further investigation of the pituitary was done. Why? • Central DI • The glucose in the NICU was low • ? Cortisol deficiency • ? Growth hormone deficiency • Result: Serum cortisol low for age
Revisit the H & P • The resident went back to spend some time examining and observing the infant. • She noted that the eyes seemed to “wander”. That is, the baby could not fix her gaze • Why? What should you do at this point? • Ophthalmology consult was obtained • Impression: Bilateral optic nerve hypoplasia
Problem Definition Revisited • So what do we have now? • Direct hyperbilirubinemia • Central Diabetes Insipidus • Cortisol deficiency • Optic Nerve Hypoplasia • Can we tie all these problems into one diagnosis?
Final Diagnosis: Septo-Optic Dysplasia (SOD)
Septo-Optic Dysplasia • One of the most common forms of congenital growth hormone deficiency • Results from incomplete development of forebrain & pituitary • Must have 2 of these 3 features for a diagnosis • Optic nerve hypoplasia • Absent septum pellucidum/corpus callosum • Pituitary endocrinopathy (deficiency) • Isolated GH deficiency • Multiple pituitary hormone deficiencies • May also see other midline defects (ex cleft lip) • MRI results widely vary
Pituitary Abnormalities • Varying degrees of endocrine disturbance seen • None • GH • TSH • LH/FSH • ACTH • Prolactin • ADH • Did you know?? • Hypopituitarism can lead to cholestasis
Clinical Features • Short stature • Precocious/ Delayed Puberty • Diabetes Insipidus (25%) • Most cases are sporadic but familial forms do occur suggesting genetic defects may play an important role • Viruses • Teratogens
Follow-up of our patient • Continued to have low cortisol (replaced) • Became hypothyroid and was started on thyroxine • Direct hyperbilirubinemia resolved with DDAVP
Take Home Messages What are your take away points?
Thanks for your participation Hope you enjoyed the puzzler and learned something new!



![[Insert Puzzler]](https://cdn3.slideserve.com/5646534/slide1-dt.jpg)

![[Insert puzzler here]](https://cdn3.slideserve.com/6623362/slide1-dt.jpg)