Download
1 / 1
10 likes | 156 Views
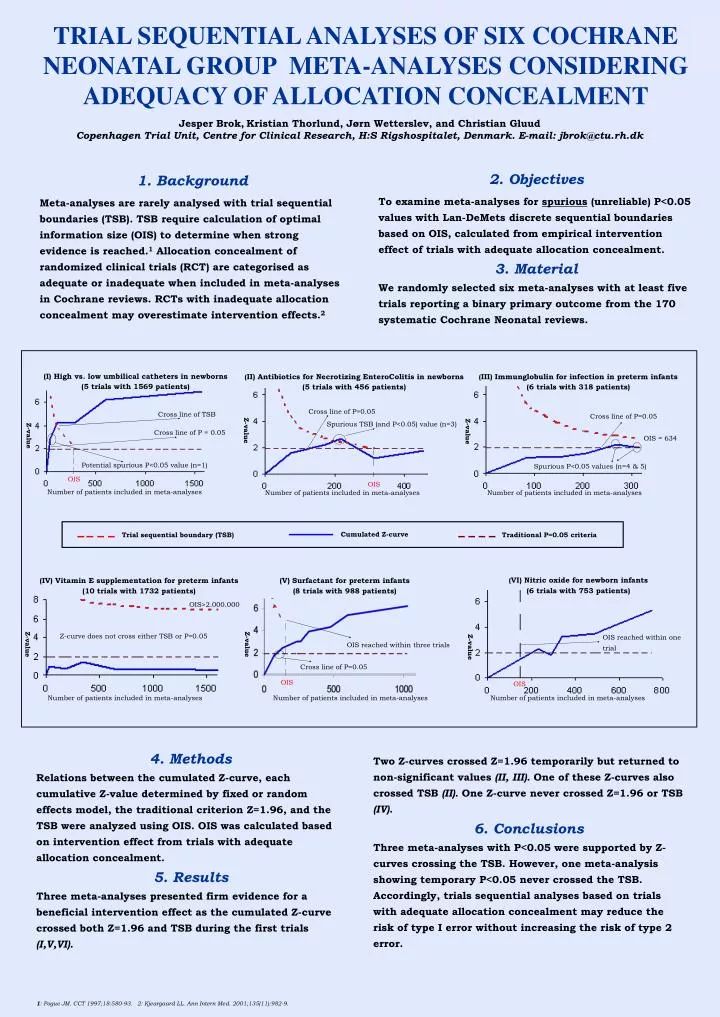
Cumulated Z-curve. Trial sequential boundary (TSB). Traditional P=0.05 criteria. TRIAL SEQUENTIAL ANALYSES OF SIX COCHRANE NEONATAL GROUP META-ANALYSES CONSIDERING ADEQUACY OF ALLOCATION CONCEALMENT. Jesper Brok , Kristian Thorlund, Jørn Wetterslev, and Christian Gluud

E N D
Cumulated Z-curve Trial sequential boundary (TSB) Traditional P=0.05 criteria TRIAL SEQUENTIAL ANALYSES OF SIX COCHRANE NEONATAL GROUP META-ANALYSES CONSIDERING ADEQUACY OF ALLOCATION CONCEALMENT Jesper Brok,Kristian Thorlund, Jørn Wetterslev, and Christian Gluud Copenhagen Trial Unit, Centre for Clinical Research, H:S Rigshospitalet, Denmark. E-mail: jbrok@ctu.rh.dk 2. Objectives To examine meta-analyses for spurious (unreliable) P<0.05 values with Lan-DeMets discrete sequential boundaries based on OIS, calculated from empirical intervention effect of trials with adequate allocation concealment. 3. Material We randomly selected six meta-analyses with at least five trials reporting a binary primary outcome from the 170 systematic Cochrane Neonatal reviews. 1. Background Meta-analyses are rarely analysed with trial sequential boundaries (TSB). TSB require calculation of optimal information size (OIS) to determine when strong evidence is reached.1 Allocation concealment of randomized clinicaltrials (RCT) are categorised as adequate or inadequate when included in meta-analyses in Cochrane reviews. RCTs with inadequate allocation concealment may overestimate intervention effects.2 (I) High vs. low umbilical catheters in newborns (5 trials with 1569 patients) (II) Antibiotics for Necrotizing EnteroColitis in newborns (5 trials with 456 patients) (III) Immunglobulin for infection in preterm infants (6 trials with 318 patients) Cross line of P=0.05 Cross line of TSB Cross line of P=0.05 Spurious TSB (and P<0.05) value (n=3) Z-value Z-value Cross line of P = 0.05 Z-value OIS = 634 Potential spurious P<0.05 value (n=1) Spurious P<0.05 values (n=4 & 5) OIS OIS Number of patients included in meta-analyses Number of patients included in meta-analyses Number of patients included in meta-analyses (VI) Nitric oxide for newborn infants (6 trials with 753 patients) (IV) Vitamin E supplementation for preterm infants (10 trials with 1732 patients) (V) Surfactant for preterm infants (8 trials with 988 patients) OIS>2.000.000 Z-curve does not cross either TSB or P=0.05 OIS reached within one trial Z-value Z-value OIS reached within three trials Z-value Cross line of P=0.05 OIS OIS Number of patients included in meta-analyses Number of patients included in meta-analyses Number of patients included in meta-analyses 4. Methods Relations between the cumulated Z-curve, each cumulative Z-value determined by fixed or random effects model, the traditional criterion Z=1.96, and the TSB were analyzed using OIS. OIS was calculated based on intervention effect from trials with adequate allocation concealment. 5. Results Three meta-analyses presented firm evidence for a beneficial intervention effect as the cumulated Z-curve crossed both Z=1.96 and TSB during the first trials (I,V,VI). Two Z-curves crossed Z=1.96 temporarily but returned to non-significant values (II, III). One of these Z-curves also crossed TSB (II). One Z-curve never crossed Z=1.96 or TSB (IV). 6. Conclusions Three meta-analyses with P<0.05 were supported by Z-curves crossing the TSB. However, one meta-analysis showing temporary P<0.05 never crossed the TSB. Accordingly, trials sequential analyses based on trials with adequate allocation concealment may reduce the risk of type I error without increasing the risk of type 2 error. 1: Pogue JM. CCT 1997;18:580-93. 2: Kjeargaard LL. Ann Intern Med. 2001;135(11):982-9.