Download
1 / 22
• 220 likes • 359 Views
Feast or Famine: Survival and Chronic Kidney Disease. Kerin Worley and Deb Gipson UNC Chapel Hill April, 2004. 1. Select the patient for whom a UNC standard renal diet is appropriate. Answer yes or no to each option:

E N D
Feast or Famine: Survival and Chronic Kidney Disease Kerin Worley and Deb Gipson UNC Chapel Hill April, 2004
1. Select the patient for whom a UNC standard renal diet is appropriate Answer yes or no to each option: A. 6 month old with posterior urethral valves and chronic renal insufficiency (eGFR 35) B. 15 year old with nephrotic syndrome (Urinary protein excretion 5 gm/day) and normal serum creatinine (0.7) C. 8 year old dependent on peritoneal dialysis D. 5 year old dependent on hemodialysis E. 11 year old with a functioning kidney transplant
1. Select the patient for whom a UNC standard renal diet is appropriate Answer yes or no to each option: A. 6 month old with posterior urethral valves and chronic renal insufficiency (eGFR 35) No B. 15 year old with nephrotic syndrome (Urinary protein excretion 5 gm/day) and normal serum creatinine (0.7) No C. 8 year old dependent on peritoneal dialysis No D. 5 year old dependent on hemodialysis No E. 11 year old with a functioning kidney transplant No
2. What are the restricted ingredients of a standard UNC Hospitals renal diet? Answer yes or no to each option: A. water B. sodium C. potassium D. phosphorus E. flavor
2. What are the restricted ingredients of a standard UNC Hospitals renal diet? Answer yes or no to each option: A. water No B. sodium Yes C. potassium Yes D. phosphorus No E. flavor :)
3. What is the proper diet for a child with dialysis dependence? Write the order please: Diet: ____________________________
4. What is the most appropriate diet for an infant with posterior urethral valves and chronic renal insufficiency (eGFR 30)? Write the order please: Diet: ____________________________
Somatic Growth in Children with CKD Impairment related to • Diminished caloric intake • Increased risk of calorie loss: GERD • Acidosis • Polyuria w/ early satiety • IGF/Growth Hormone Axis disturbance • Age of onset of CKD • Severity of renal failure • co-morbidities/syndromes
How do our children grow?NAPRTCS 2003 ADR: CRI Registry Ht SDS Entry 12 24 36 Time (months)
Weight and CRINAPRTCS 2003 ADR: CRI Registry Weight SDS entry 12m 24 m 36 m
Growth and Dialysis in ChildrenNAPRTCS 2003 ADR: Dialysis Registry Entry Month 12 Month 24 Weight SDS Age 0-1 -2.36 -1.83 -1.30 2-5 -1.28 -1.32 -1.21 6-12 -1.26 -1.24 -1.42 >12 -1.00 -1.02 -1.28 Height SDS Age 0-1 -2.52 -2.31 -2.12 2-5 -1.99 -2.24 -2.03 6-12 -1.75 -1.89 -2.17 >12 -1.33 -1.45 -1.59
Nutritional Focus: 1985 and beyondUSRDS, 2001 ADR Death rates on dialysis for children age 0-19 Hemodialysis Year 1: 29/1000 patient years Year 2: 32/ 1000 patient years Peritoneal Dialysis Year 1: 60 / 1000 patient years Year 2: 34 / 1000 patient years
Hypoalbuminemia and Survival in ESRDC. Wong, Kidney Int. 61, 2002 • Incident dialysis patients 1995 - 1998 • N=1723 • Age 0-18 years • Outcome: mortality • 93 deaths over 2953 patient-years observed Mortality rate of 31.5 / 1000 pt years
Hypoalbuminemia and Survival in ESRDC. Wong, Kidney Int. 61, 2002 Mortality Risk Albumin < 3.5 g/dL RR 1.90 (1.16, 3.10) Adjusted for gender, age, race, modality, etiology of esrd, height sds and wt sds Insert fig 1 c. wong 2002 ki
Prevalence of Protein MalnutritionA. Brem, P. Nephrol, 2002 • Given hypoalbuminemia is a surrogate for mortality risk • Question the prevalence of serum albumin<2.9 in • children PD • children HD • adults PD • Assess nutritional protein intake
Prevalence of Protein MalnutritionA. Brem, P. Nephrol, 2002 Dietary protein intake is assessed as Protein Catabolic Rate (PCR). National dialysis guidelines recommend PCR of 1g/kg/day (KDOQI)
Correlates of Protein Malnutrition in ChildrenA. Brem, P. Nephrol, 2002 S Alb at dialysis initiation correlates with future hypoalbuminemia risk Relationship between Inflammation and S Alb
CKD Severity and NutritionL Norman, P Nephrol. 15, 2000 GFR N Age RD consult Cal Intake(% Goal) > 75 35 8.2 3% 103 50-75 23 8.2 13% 99 25-49 19 8.5 37% 92 <25 61 10.2 61% 85 Insert figure 1 Comparison of anthros and CKD severity
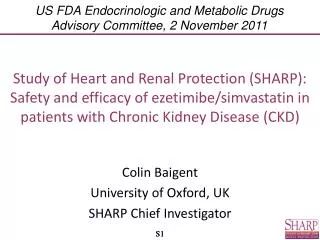
CKD and BMI: The big UC. Wong, AJKD 36, 2000 N=1949 Prevalent ESRD All Modes ‘89-’91 aRR for Death BMI Standard Deviation Score P=0.001
Dietary protein and progressive CKD • Adults (Klahr, NEJM, 1994) • Modification of Diet in Renal Disease Study (MDRD) • RCT of protein restriction • Inclusion GFR 25 - 55ml/min • Usual diet (P 1.3 g/d) vs Low diet (P 0.58 g/d) • 2-3 years follow up • GFR decline ~ 5 ml/min/yr in both • Pediatrics • Dietary protein intake to RDA / optimize nutritional status • No association between protein restriction and CKD progression in small studies
Distribution of height SDS of 1949 patients compared with children in US general population Wong CS et al. Am J Kidney Dis 2000; 36(4):811-819