Download
1 / 1

E N D
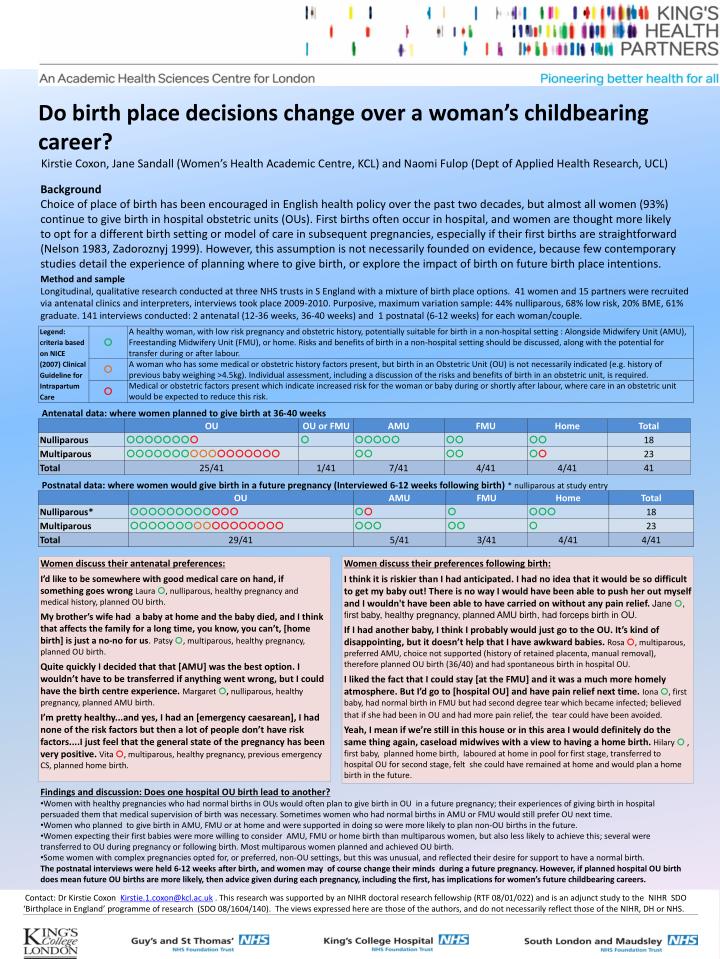
BackgroundChoice of place of birth has been encouraged in English health policy over the past two decades, but almost all women (93%) continue to give birth in hospital obstetric units (OUs). First births often occur in hospital, and women are thought more likely to opt for a different birth setting or model of care in subsequent pregnancies, especially if their first births are straightforward (Nelson 1983, Zadoroznyj 1999). However, this assumption is not necessarily founded on evidence, because few contemporary studies detail the experience of planning where to give birth, or explore the impact of birth on future birth place intentions. Method and sample Longitudinal, qualitative research conducted at three NHS trusts in S England with a mixture of birth place options. 41 women and 15 partners were recruited via antenatal clinics and interpreters, interviews took place 2009-2010. Purposive, maximum variation sample: 44% nulliparous, 68% low risk, 20% BME, 61% graduate. 141 interviews conducted: 2 antenatal (12-36 weeks, 36-40 weeks) and 1 postnatal (6-12 weeks) for each woman/couple. Do birth place decisions change over a woman’s childbearing career?Kirstie Coxon, Jane Sandall (Women’s Health Academic Centre, KCL) and Naomi Fulop (Dept of Applied Health Research, UCL) Antenatal data: where women planned to give birth at 36-40 weeks Postnatal data: where women would give birth in a future pregnancy (Interviewed 6-12 weeks following birth)* nulliparous at study entry Women discuss their antenatal preferences: I’d like to be somewhere with good medical care on hand, if something goes wrong Laura , nulliparous, healthy pregnancy and medical history, planned OU birth. My brother’s wife had a baby at home and the baby died, and I think that affects the family for a long time, you know, you can’t, [home birth] is just a no-no for us.Patsy , multiparous, healthy pregnancy, planned OU birth. Quite quickly I decided that that [AMU] was the best option. I wouldn’t have to be transferred if anything went wrong, but I could have the birth centre experience. Margaret ,nulliparous, healthy pregnancy, planned AMU birth. I’m pretty healthy...and yes, I had an [emergency caesarean], I had none of the risk factors but then a lot of people don’t have risk factors....I just feel that the general state of the pregnancy has been very positive. Vita , multiparous, healthy pregnancy, previous emergency CS, planned home birth. Women discuss their preferences following birth: I think it is riskier than I had anticipated. I had no idea that it would be so difficult to get my baby out! There is no way I would have been able to push her out myself and I wouldn't have been able to have carried on without any pain relief. Jane , first baby, healthy pregnancy, planned AMU birth, had forceps birth in OU. If I had another baby, I think I probably would just go to the OU. It’s kind of disappointing, but it doesn’t help that I have awkward babies. Rosa , multiparous, preferred AMU, choice not supported (history of retained placenta, manual removal), therefore planned OU birth (36/40) and had spontaneous birth in hospital OU. I liked the fact that I could stay [at the FMU] and it was a much more homely atmosphere. But I’d go to [hospital OU] and have pain relief next time. Iona , first baby, had normal birth in FMU but had second degree tear which became infected; believed that if she had been in OU and had more pain relief, the tear could have been avoided. Yeah, I mean if we’re still in this house or in this area I would definitely do the same thing again, caseload midwives with a view to having a home birth. Hilary , first baby, planned home birth, laboured at home in pool for first stage, transferred to hospital OU for second stage, felt she could have remained at home and would plan a home birth in the future. • Findings and discussion: Does one hospital OU birth lead to another? • Women with healthy pregnancies who had normal births in OUs would often plan to give birth in OU in a future pregnancy; their experiences of giving birth in hospital persuaded them that medical supervision of birth was necessary. Sometimes women who had normal births in AMU or FMU would still prefer OU next time. • Women who planned to give birth in AMU, FMU or at home and were supported in doing so were more likely to plan non-OU births in the future. • Women expecting their first babies were more willing to consider AMU, FMU or home birth than multiparous women, but also less likely to achieve this; several were transferred to OU during pregnancy or following birth. Most multiparous women planned and achieved OU birth. • Some women with complex pregnancies opted for, or preferred, non-OU settings, but this was unusual, and reflected their desire for support to have a normal birth. • The postnatal interviews were held 6-12 weeks after birth, and women may of course change their minds during a future pregnancy. However, if planned hospital OU birth does mean future OU births are more likely, then advice given during each pregnancy, including the first, has implications for women’s future childbearing careers. Contact: Dr Kirstie Coxon Kirstie.1.coxon@kcl.ac.uk . This research was supported by an NIHR doctoral research fellowship (RTF 08/01/022) and is an adjunct study to the NIHR SDO ‘Birthplace in England’ programme of research (SDO 08/1604/140). The views expressed here are those of the authors, and do not necessarily reflect those of the NIHR, DH or NHS.