Download
1 / 1
10 likes | 131 Views
INTRODUCTION 50% PATIENTS WITH CURATIVE SURGERY DIE WITHIN 5YEARS CHEMOTHERAPY INEFFECTIVE IN DUKES B (IMPACT B2 TRIAL) (But would benefit those 30% destined to relapse) NEED TO IDENTIFY THOSE DUKES B PATIENTS DESTINED TO RELAPSE ? INACCURATE STAGING, ? DETECTION OF MICROMETASTASES.

E N D
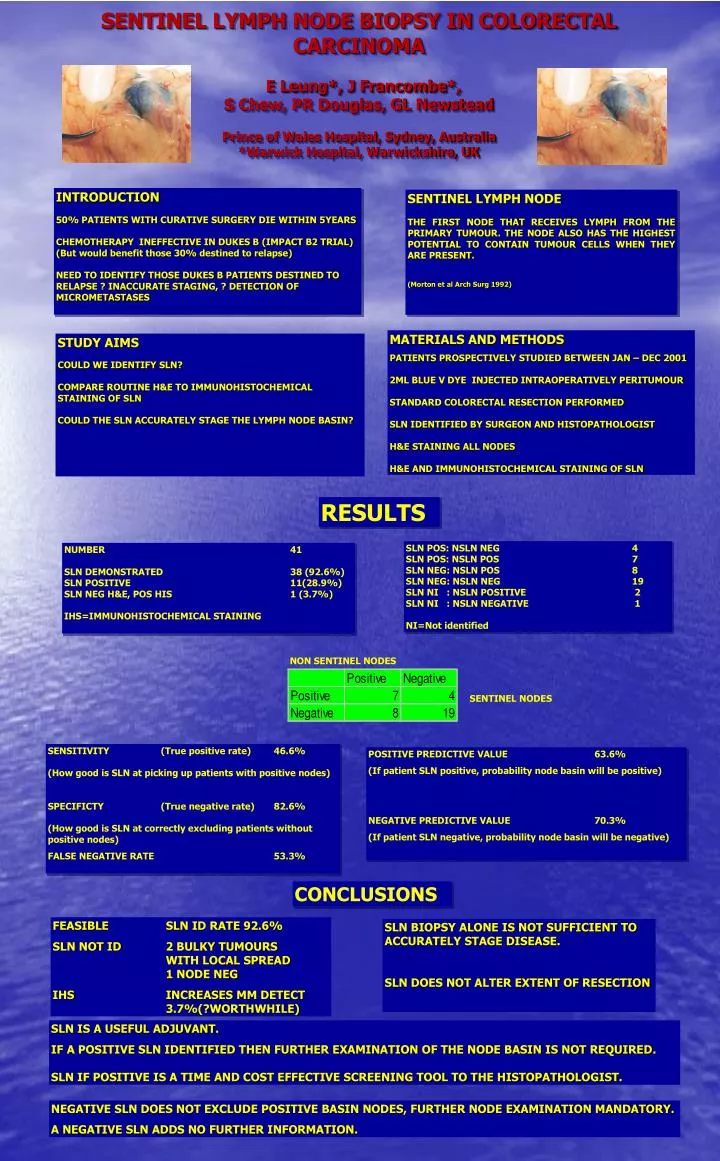
INTRODUCTION 50% PATIENTS WITH CURATIVE SURGERY DIE WITHIN 5YEARS CHEMOTHERAPY INEFFECTIVE IN DUKES B (IMPACT B2 TRIAL) (But would benefit those 30% destined to relapse) NEED TO IDENTIFY THOSE DUKES B PATIENTS DESTINED TO RELAPSE ? INACCURATE STAGING, ? DETECTION OF MICROMETASTASES SENTINEL LYMPH NODE THE FIRST NODE THAT RECEIVES LYMPH FROM THE PRIMARY TUMOUR. THE NODE ALSO HAS THE HIGHEST POTENTIAL TO CONTAIN TUMOUR CELLS WHEN THEY ARE PRESENT. (Morton et al Arch Surg 1992) MATERIALS AND METHODS PATIENTS PROSPECTIVELY STUDIED BETWEEN JAN – DEC 2001 2ML BLUE V DYE INJECTED INTRAOPERATIVELY PERITUMOUR STANDARD COLORECTAL RESECTION PERFORMED SLN IDENTIFIED BY SURGEON AND HISTOPATHOLOGIST H&E STAINING ALL NODES H&E AND IMMUNOHISTOCHEMICAL STAINING OF SLN STUDY AIMS COULD WE IDENTIFY SLN? COMPARE ROUTINE H&E TO IMMUNOHISTOCHEMICAL STAINING OF SLN COULD THE SLN ACCURATELY STAGE THE LYMPH NODE BASIN? SENTINEL LYMPH NODE BIOPSY IN COLORECTAL CARCINOMA E Leung*, J Francombe*, S Chew, PR Douglas, GL NewsteadPrince of Wales Hospital, Sydney, Australia *Warwick Hospital, Warwickshire, UK RESULTS SLN POS: NSLN NEG 4 SLN POS: NSLN POS 7 SLN NEG: NSLN POS 8 SLN NEG: NSLN NEG 19 SLN NI : NSLN POSITIVE 2 SLN NI : NSLN NEGATIVE 1 NI=Not identified NUMBER 41 SLN DEMONSTRATED 38 (92.6%) SLN POSITIVE 11(28.9%) SLN NEG H&E, POS HIS 1 (3.7%) IHS=IMMUNOHISTOCHEMICAL STAINING NON SENTINEL NODES SENTINEL NODES SENSITIVITY (True positive rate) 46.6% (How good is SLN at picking up patients with positive nodes) SPECIFICTY (True negative rate) 82.6% (How good is SLN at correctly excluding patients without positive nodes) FALSE NEGATIVE RATE 53.3% POSITIVE PREDICTIVE VALUE 63.6% (If patient SLN positive, probability node basin will be positive) NEGATIVE PREDICTIVE VALUE 70.3% (If patient SLN negative, probability node basin will be negative) CONCLUSIONS FEASIBLE SLN ID RATE 92.6% SLN NOT ID 2 BULKY TUMOURS WITH LOCAL SPREAD 1 NODE NEG IHS INCREASES MM DETECT 3.7%(?WORTHWHILE) SLN BIOPSY ALONE IS NOT SUFFICIENT TO ACCURATELY STAGE DISEASE. SLN DOES NOT ALTER EXTENT OF RESECTION SLN IS A USEFUL ADJUVANT. IF A POSITIVE SLN IDENTIFIED THEN FURTHER EXAMINATION OF THE NODE BASIN IS NOT REQUIRED. SLN IF POSITIVE IS A TIME AND COST EFFECTIVE SCREENING TOOL TO THE HISTOPATHOLOGIST. NEGATIVE SLN DOES NOT EXCLUDE POSITIVE BASIN NODES, FURTHER NODE EXAMINATION MANDATORY. A NEGATIVE SLN ADDS NO FURTHER INFORMATION.