Download
1 / 1
10 likes | 221 Views
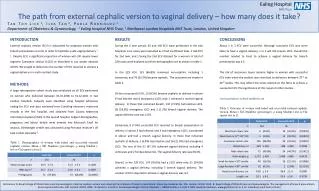
Ealing Hospital NHS Trust Service Evaluation of Laparoscopic and Hysteroscopic Sterilisation Asmaa Al- Kufaishi 1 , Seosoon Seah 2 , Tan Toh Lick 1 Department of Obstetrics & Gynaecology 1 and Anaesthetics 2 , Ealing Hospital NHS Trust, London, United Kingdom. INTRODUCTION

E N D
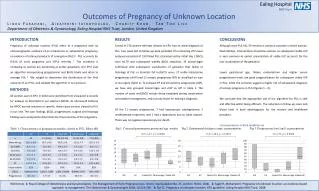
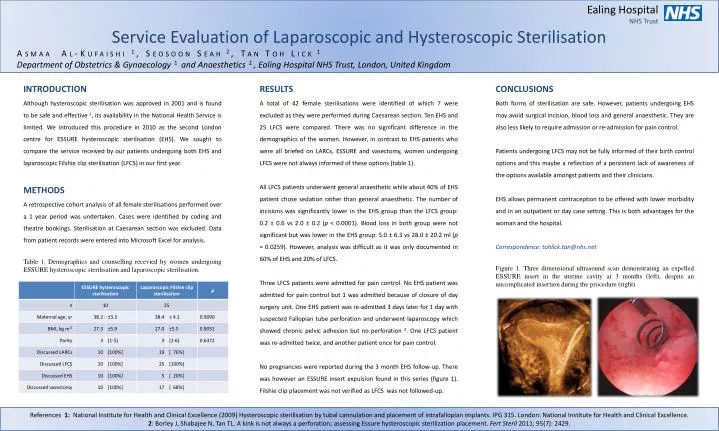
Ealing Hospital NHS Trust Service Evaluation of Laparoscopic and Hysteroscopic Sterilisation Asmaa Al-Kufaishi1, Seosoon Seah 2, Tan Toh Lick 1 Department of Obstetrics & Gynaecology 1 and Anaesthetics 2, Ealing Hospital NHS Trust, London, United Kingdom INTRODUCTION Although hysteroscopic sterilisation was approved in 2001 and is found to be safe and effective 1, its availability in the National Health Service is limited. We introduced this procedure in 2010 as the second London centre for ESSURE hysteroscopic sterilisation (EHS). We sought to compare the service received by our patients undergoing both EHS and laparoscopic Filshie clip sterilisation (LFCS) in our first year. METHODS A retrospective cohort analysis of all female sterilisations performed over a 1 year period was undertaken. Cases were identified by coding and theatre bookings. Sterilisation at Caesarean section was excluded. Data from patient records were entered into Microsoft Excel for analysis. Table 1. Demographics and counselling recevied by women undergoing ESSURE hysteroscopic sterilisation and laparoscopic sterilisation. RESULTS A total of 42 female sterilisations were identified of which 7 were excluded as they were performed during Caesarean section. Ten EHS and 25 LFCS were compared. There was no significant difference in the demographics of the women. However, in contrast to EHS patients who were all briefed on LARCs, ESSURE and vasectomy, women undergoing LFCS were not always informed of these options (table 1). All LFCS patients underwent general anaesthetic while about 40% of EHS patient chose sedation rather than general anaesthetic. The number of incisions was significantly lower in the EHS group than the LFCS group: 0.2 ± 0.6 vs 2.0 ± 0.2 (p < 0.0001). Blood loss in both group were not significant but was lower in the EHS group: 5.0 ± 6.3 vs 28.0 ± 20.2 ml (p = 0.0259). However, analysis was difficult as it was only documented in 60% of EHS and 20% of LFCS. Three LFCS patients were admitted for pain control. No EHS patient was admitted for pain control but 1 was admitted because of closure of day surgery unit. One EHS patient was re-admitted 3 days later for 1 day with suspected Fallopian tube perforation and underwent laparoscopy which showed chronic pelvic adhesion but no perforation 2. One LFCS patient was re-admitted twice, and another patient once for pain control. No pregnancies were reported during the 3 month EHS follow-up. There was however an ESSURE insert expulsion found in this series (figure 1). Filshie clip placement was not verified as LFCS was not followed-up. CONCLUSIONS Both forms of sterilisation are safe. However, patients undergoing EHS may avoid surgical incision, blood loss and general anaesthetic. They are also less likely to require admission or re-admission for pain control. Patients undergoing LFCS may not be fully informed of their birth control options and this maybe a reflection of a persistent lack of awareness of the options available amongst patients and their clinicians. EHS allows permanent contraception to be offered with lower morbidity and in an outpatient or day case setting. This is both advantages for the woman and the hospital. Correspondence: tohlick.tan@nhs.net Figure 1. Three dimensional ultrasound scan demonstrating an expelled ESSURE insert in the uterine cavity at 3 months (left), despite an uncomplicated insertion during the procedure (right). References 1: National Institute for Health and Clinical Excellence (2009) Hysteroscopic sterilisation by tubal cannulation and placement of intrafallopian implants. IPG 315. London: National Institute for Health and Clinical Excellence. 2: Borley J, Shabajee N, Tan TL. A kink is not always a perforation; assessing Essurehysteroscopic sterilization placement.FertSteril 2011; 95(7): 2429.