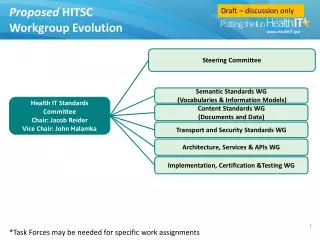
Download
1 / 8
80 likes | 211 Views
HITSC Implementation Workgroup. July 28, 2014. Quality Data Measurement Is An End-to-End Process. Electronic reporting MU, PQRS , AQC , etc. Documentation & extraction. Transport. Validation and analysis. User access. Data management Report viewing Case tracking. RX Labs Vitals

E N D
HITSC Implementation Workgroup July 28, 2014
Quality Data Measurement Is An End-to-End Process • Electronic reporting • MU, PQRS, AQC, etc Documentation & extraction Transport Validation and analysis User access • Data management • Report viewing • Case tracking RX Labs Vitals Problems Patient Provider Payer etc HIE Web services TCPIP SFTP Other Clinical source system • Data extraction • Queries • Pre-defined data marts • Management Info System • User information • Utilization analysis • Other Remediation and Improvement
QDC Analytics Measure Inventory Government Commercial PCMH MU Stage 1 and 2 EP and EH PQRS Pioneer ACO
Data Sources Clinical Claims
CCDA has been workable, but it is cumbersome • From a technical perspective, it’s an unwieldy container, but these issues can be overcome • CCDA architecture provides framework for standardized document-representation structured data • Biggest issue is wide implementation variation across EHR vendors • Two types of variation • Data availability • One CCDA does not fit all needs • Some clinical information not available in CCDAs with certain vendors due to timing of CCDA generation in workflow • e.g, Labs and E&M codes not included in CCDAs that get generated at end of visits • Data introduced for MU Stage 2 CQMs not available or not standardized among vendors (e.g., patient communication codes, devices applied on patients, reasons for not performing intervention, etc) • Semantic normalization • Some fields are rough but often can be remediated (problems, medications, vitals, labs) vendor-by-vendor • Other fields are often not available or non-standardized across systems (historical procedure information, social history for codes on smoking status, cessation counseling, etc)
Recommendations • Availability of standardized templates and implementation guides for high frequency and high value use cases • ambulatory visit, inpatient visit, ED visit, specialist referral, nursing home TOC, HIE data aggregation, quality data aggregation, etc • Current work in CCDA templates and FHIR profiles is working on this, but needs to be aggressively accelerated and made available • Certification testing focused more specifically on implementation of CCDA to support data availability and semantic normalization for high priority use cases
Informationwww.maehc.orgMicky Tripathi, PhD MPPPresident & CEOmtripathi@maehc.org781-434-7906