Download

1 / 20
220 likes | 460 Views
Corticoids. Lindsey Elmore Lindsey.elmore@ucsf.edu. Objectives. Describe the HPA axis Describe cholesterol conversion to aldosterone and cortisol Identify metabolites of cortisol, aldosterone and synthetic agonists and predict how modifications affect biotransformations

E N D
Corticoids Lindsey Elmore Lindsey.elmore@ucsf.edu
Objectives • Describe the HPA axis • Describe cholesterol conversion to aldosterone and cortisol • Identify metabolites of cortisol, aldosterone and synthetic agonists and predict how modifications affect biotransformations • Be able to recognize name and MOA of mineralocorticoid agonists and antagonists • Be familiar with side effects with anti-inflammatory drugs and the rationale for tapering
Objectives • Be able to discuss absorption, transport, metabolic rate and receptor binding affinity and how that influences biometabolic effects • Know the administration routes for corticoids • Be able to predict the changes in activity for the six most common structural changes. • Know the name and MOA of antagonists.
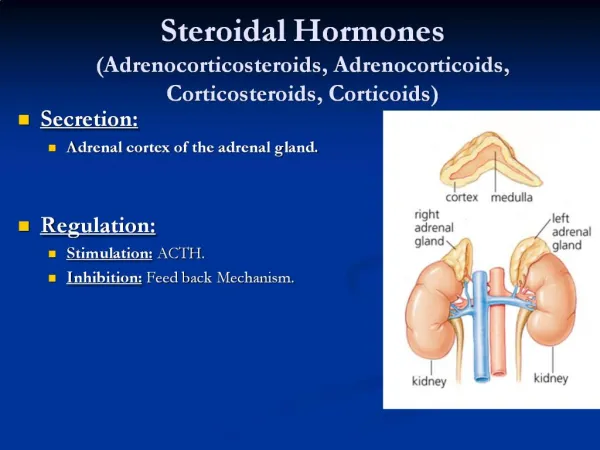
Hypothalamus-Pituitary-Adrenal axis is a negative feedback system where cortisol and other steroids inhibit their own metabolism. Disturbances in the HPA axis Describe the HPA axis
Corticosteroids are regulated by corticotropin releasing hormone which is a small protein. Corticoids have a wide range of physiological actions including effects on metabolism and salt retention, and receptors on almost every cell in the body. Describe the HPA axis
Under normal, non-stressful conditions about 20 mg/day of cortisol is released. In congenital adrenal hyperplasia there is a defect in cortisol production and negative feedback is lost. Supplementation must be taken. Cushing’s disease increases cortisol production and decreases the amount of ACTH produced because of negative feedback. Patients with drug induced Cushing’s must slowly taper meds. Describe the HPA axis
All steroids are derived from cholesterol, and the production of pregneolone is the rate limiting step in the production of steroids. In the adrenals, aldosterone is produced. Describe cholesterol conversion to aldosterone and cortisol
Cortisol and cortisone are interconverted by 11B-HSD in the liver with the equilibrium lying towards cortisol. Cortisol is the most active human glucocorticoid and cortisone is inactive, but can be reactivated through reverse activation. Overexpression of 11B-HSD leads to Cushing’s fat deposits and metabolic disease. Aldosterone is the predominant mineralocorticoid, and the 18-aldehyde exists in a hemi-acetal form to prevent oxidative degradation. Describe cholesterol conversion to aldosterone and cortisol base acid
Corticoids are not stored, but are synthesized on demand from cholesterol esters. Most congenital adrenal hyperplasias involve lack of 21 B or 11B hydroxylase. Blockade of other pathways leads to overproduction of aldosterone. Describe cholesterol conversion to aldosterone and cortisol 17a-OH 21 OH 3B 17OH dehydro-genase 3 B OH dehydrogenase
Metabolized mostly by the liver. Synthetic steroids are generally metabolized the same way, but at a much slower rate (especially those with 6 and 16 substituents. Identify metabolites of cortisol, aldosterone and synthetic agonists and predict how modifications affect biotransformations Major pathway inactive inactive inactive
There are dozens of metabolites of cortisol. Know the main ones. Identify metabolites of cortisol, aldosterone and synthetic agonists and predict how modifications affect biotransformations 20 ketone reduction A ring reduction 17 oxidative removal of side chain
Be able to recognize name and MOA of mineralocorticoid agonists and antagonists • Agonists are rarely used and are usually only for congenital defects or to increase circulating volume, • Fludrocortisone is very potent possessing 800x the MC activity and 11x the GC activity of cortisol. Used to treat adrenal insufficiency and to increase circulating volume. Desoxycorticosterone is not very useful because it cannot be given po and has fallen out of favor.
Be able to recognize name and MOA of mineralocorticoid agonists and antagonists • Spironolactone and eplerenone are aldosterone receptor antagonists and are useful in the treatment of hypertension. Spironolactone also has diuretic activity.
Be familiar with side effects with anti-inflammatory drugs and the rationale for tapering • Use corticoids to treat adrenal disfunction or hyperfunction, to stimulate fetal lung maturation, and in non-endocrine diseases such as inflammatory processes and cancer.
Be familiar with side effects with anti-inflammatory drugs and the rationale for tapering • One of the most important side effects of corticoid therapy is that it suppresses the production of endogenous corticoids. • The effect is dose related and duration related. Exogenous corticosteroids inhibit the release of CRF and therefore ACTH and adrenals atrophy and circulating cortisol decreases. • Abruptly discontinuing steroids can be life threatening because of severe hypotension, and therapy must be tapered very slowly to allow adrenals to increase production of steroids. • Use lowest dose possible for the shortest amount of time in order to curtail side effects.
Be able to discuss absorption, transport, metabolic rate and receptor binding affinity and how that influences biometabolic effects • Absorption: 21 esters, C3 sulfates, and 16,17acetonides decrease lipophilicity. The more lipophilic the drug is the more likely that it can be given po. • Distribution: 17 Me decreases protein binding • Metabolism 17 a increses t1/2 by preventing oxidation
Topical Topical administration requires high degree of lipophilicity. Drugs that are not very lipophilic can be esterified to increase absorption through the stratum corneum. Occluding the wound can also increase systemic absorption and lead to side effects. But if you increase lipophilicity too much the drug will not be able to flux out of the skin as is seen with large esters like palmitate (16 carbons). So, in order for a drug to be topically active there must be a balance of hydrophilicity and hydrophobicity. Know the administration routes for corticoids
Know the administration routes for corticoids • Intraarticluar: Aqueous suspensions of microcrystalline esters • Opthalmic: Moderate hydrophobicity (acetates) • IV: Need enough hydrophilicity to go into solution so use water soluble esters
Know how the modifications change activity. This chart is your friend. Be able to predict the changes in activity for the six most common structural changes.
Two classes of antagonists: synthesis inhibitors and receptor antagonists. Aminoglutethimide inhibits the rate determining step in steroid biosynthesis. Metyrapone inhibits 11B OH and is used for diagnosis. Ketoconazole inhibits everything. Know the name and MOA of antagonists.