Download
1 / 21
210 likes | 446 Views
Anti-Malaria Drug Policy Philippines. Workshop on Anti-Malarial Drug Policy Implementation Review Wuxi City, Jiangsu Provincial Institute of Parasitic Diseases, P.R. China September 12 – 22, 2005. GEOGRAPHICAL DISTRIBUTION OF MALARIA PHILIPPINES ( Based on 10-year Average, 1991 – 2000 ).

E N D
Anti-Malaria Drug PolicyPhilippines Workshop on Anti-Malarial Drug Policy Implementation Review Wuxi City, Jiangsu Provincial Institute of Parasitic Diseases, P.R. China September 12 – 22, 2005
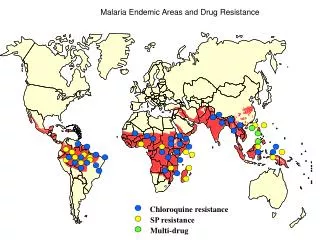
GEOGRAPHICAL DISTRIBUTION OF MALARIA PHILIPPINES ( Based on 10-year Average, 1991 – 2000 ) • Category A Provinces • 25 Provinces • more than 1000 cases/year or • situation worsened • Category B Provinces • 22 Provinces • 100 to < 1000 cases/year or • situation has improved in the last 5 yrs • Category C Provinces • 18 Provinces • less than 100 cases/year • Category D Provinces • 13 provinces • Malaria-free (no more indigenous cases for at least 3 years Source: Malaria Control Program, 2000 Department of Health
Malaria Drug Policy (DOH Administrative Order No.129-A) MCP-DOHDate: August 23, 2002 “Previous” Drug Policy 1st line: Chloroquine 2nd line: Sulfadoxine-Pyrimethamine (SP) 3rd line: Quinine + Primaquine New Drug Policy 1st line: CQ+SP 2nd line: Artemether + lumefantrine [Coartem™ ] 3rd line: Quinine + anti- biotic (Tetracycline, clinda, doxy, erythro) + Primaquine
> 25% 16 - 24% 6- 15% < 5% Basis for Changing treatment policy DRUG TREATMENT FAILURE RATES in the Philippines, 2000 Treatment Failure Rate CQ >>> 25% SP > 25% (MCS, 1996-1997; Preliminary Report ENHR, 2000; ADS-MCP, 1997-2000; WHO-RBM, 2000-2001)
Chloroquine (CQ) and Sulfadoxine-Pyrimethamine (SP) Drug Profile in Selected Study Sites, Philippines • Kal-Apayao (2000) CQ > 42% Tx F SP > 9% Tx F • Palawan (1994-2000) • CQ 39-76% Tx F • SP 12.5-20% TxF • Davao N-ComVal (2000) • Agusan del Sur (97-01) CQ > 50% Tx F SP > 43% Tx F
This high treatment failure rates provide a very strong evidence for the DOH to immediately review & change existing anti-malarial drug policy in the country.Combination therapy becomes a more viable alternative in improving efficacy of available drugs.
Combination CQ+SP vs Coartem™ , Agusan del Sur and Compostela Valley, Philippines, 2001 - therapeutic efficacy surveillance done in small population to predict outcome of treatment in known drug resistant areas Study Site Drugs N 28-day Tx F Cure Rate ADS CQ+SP 39 36 4 89% (32/36) SP 35 32 17 47% (15/35) Laac, CV CQ+SP 40 38 7 82% (31/38) Coartem 40 36 0 100% Espino et al, 2001. Preliminary report, WHO/RBM-ADS/MCP
Malaria Drug Policy (A.O.129-A) MCP-DOH • 100% efficacy of A-L combination, however restricted to be used as 2nd line drug bec. of: • limited findings of its safety for very young children, pregnant women & breastfeeding mothers. • Inadequate capability of the current health infrastructure in many endemic areas to provide confirmatory diagnosis. • DOH: more time to explore & further study the use of artemisinin-based combinations before it is adopted as 1st line drug
Malaria Drug Policy (A.O.129-A) MCP-DOH • Provides policies & guidelines for diagnosis and combination chemotherapy for malaria • Objective: • Further reduce the development of drug resistance & ultimately towards reducing morbidity & transmission & preventing complications & malaria deaths
Malaria Drug Policy (A.O.129-A) MCP-DOH • Coverage: • All government (national and local) and private health facilities nationwide
Malaria Drug Policy (A.O.129-A) MCP-DOH • Implementation: • To be implemented in phases • Why? • - NMCP to manage the increase in cost of diagnosis & treatment • - Centers for Health Development (15 Regional Health Offices) to strengthen & expand its capacity for implementation
Malaria Drug Policy (A.O.129-A) MCP-DOH • Implementation: • Priority 1: • - Project sites where capacity building for drug policy implementation has already been carried out/underway • - Malaria microscopy centers at the Rural Health Units are already established/upgraded • Priority 2: Category A provinces (GFATM-MC) • Priority 3: Category B provinces • Priority 4: all other endemic provinces
Components of Phil. Malaria Control Program Drug Policy • Anti-malarial drug list according to use & guidelines for drug use - Combination treatment for P. falciparum malaria uncomplicated: 1st line: CQ+SP 2nd line: Artemether-Lumefantrine 3rd line: Quinine + T/D severe: QN + T/D/Clinda + Primaquine (single dose) - Tx for P. vivax malaria (CQ + Prima) - Tx for mixed infection (CQ+SP+Prima) - Tx for pregnant women & children <1 y.o. (QN) - chemoprophylaxis (Doxy/mefloquine)
Components of Phil. Malaria Control Program Drug Policy •Diagnosis (laboratory confirmation – Microscopy/RDT) - QA/AS – microscopy pilot-test - QA/AS – RDT (future plan) • Regulations for treatment & provision of drugs - all probable & confirmed malaria using 1st line – administered by trained field health workers - Tx of P. falciparum & severe/complicated malaria using A-L & QN+T/D – only dispensed by a physician/PHN upon lab. confirmation - supervised Tx (ST) shall be adopted - referral of patients (i.e. indications of severe malaria, pregnant women, children < 5 y.o.) using the existing referral system
Components of Phil. Malaria Control Program Drug Policy - Tx in outbreaks emergency situation: P. falciparum: A-L, + prima (ensure rapid cure w/ lowest risk of Tx failure P. vivax: CQ + prima • Support Systems: - Health Human Resource Dev’t: Re-training of health personnel - Logistics Mgt. System (ensure continuous supply of drugs, lab. supplies, under/over-stocking, drug expiration, etc) a) provision of 1st line drugs & lab. supplies – shared responsibility of DOH-Centers for Health Devt & Local Govt Units b) Sourcing out of funds & provision of 2nd & 3rd line drugs: Central Office, DOH c )Distribution mechanism – to ensure proper allocation & availability of drugs, supplies
Components of Phil. Malaria Control Program Drug Policy - Reporting & Surveillance System • Roles & Responsibilities - Identified roles of the National, Regional, LGU (Provl Health Office, Rural Health Units, Village Health Workers, other volunteers), NGOs • Regulations on QA & monitoring of Tx efficacy - Re-training of all health personnel /institutions - Established sentinel sites to conduct therapeutic efficacy studies
> 25% 16 - 24% 6- 15% < 5% Current Treatment Failure Rate to CQ+SP as first-line drug >15% COARTEM 100% Efficacy DRUG TREATMENT FAILURE RATES, Philippines, 2002
CQ+SP and Coartem™ Efficacy in Selected Study Sites Philippines, 2001-2004 • Kalinga & Isabela 2004 CQ+SP 94% ACPR AL 98-100% • Palawan, 1995 CQ+SP 87%ACPR 2005 on-going TES • Com Val & ADS, 2001 CQ+SP 85% ACPR AL 100% ACPR 2005 on-going TES
Current Situation: First line drug CQ+SP with 85% efficacy in some areas (interim policy until when?) Tasks at Hand: Use drugs wisely to prolong their useful lifespan - Retrain health personnel on new drug policy - Improve diagnosis, improve compliance (ST) - Train hospital-based MDs on case management Monitor drug efficacy at sentinel sites
Monitoring drug efficacy and post-marketing surveillance Treatment response to recommended drugs being monitored in sentinel sites to detect signs of decreasing drug susceptibility Supervised treatment and laboratory diagnosis needed to avoid misuse of drugs Post-marketing surveillance to identify problems related to adverse reactions, stability, quality and drug efficacy