Download
1 / 1
10 likes | 142 Views
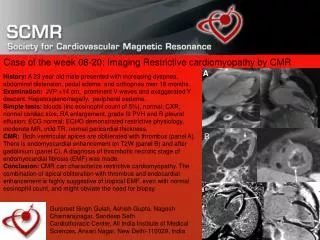
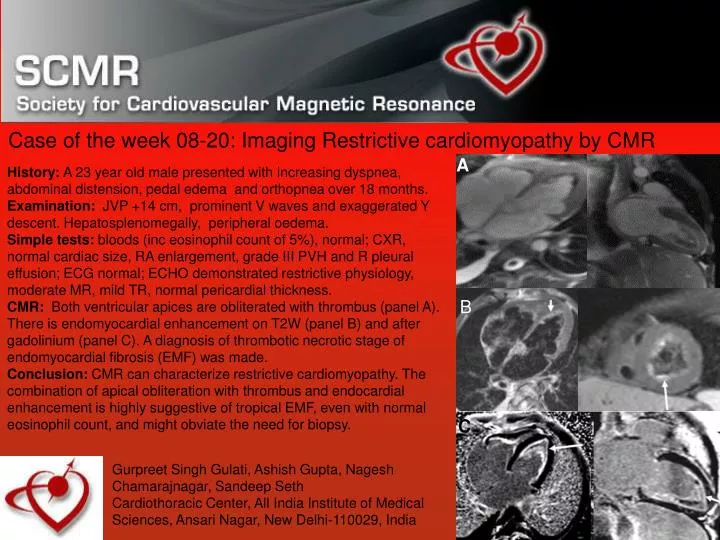
A. History: A 23 year old male presented with increasing dyspnea, abdominal distension, pedal edema and orthopnea over 18 months. Examination: JVP +14 cm, prominent V waves and exaggerated Y descent. Hepatosplenomegally, peripheral oedema.

E N D
A History: A 23 year old male presented with increasing dyspnea, abdominal distension, pedal edema and orthopnea over 18 months. Examination: JVP +14 cm, prominent V waves and exaggerated Y descent. Hepatosplenomegally, peripheral oedema. Simple tests: bloods (inc eosinophil count of 5%), normal; CXR, normal cardiac size, RA enlargement, grade III PVH and R pleural effusion; ECG normal; ECHO demonstrated restrictive physiology, moderate MR, mild TR, normal pericardial thickness. CMR:Both ventricular apices are obliterated with thrombus (panel A). There is endomyocardial enhancement on T2W (panel B) and after gadolinium (panel C). A diagnosis of thrombotic necrotic stage of endomyocardial fibrosis (EMF) was made. Conclusion: CMR can characterize restrictive cardiomyopathy. The combination of apical obliteration with thrombus and endocardial enhancement is highly suggestive of tropical EMF, even with normal eosinophil count, and might obviate the need for biopsy. Case of the week 08-20: Imaging Restrictive cardiomyopathy by CMR B C Gurpreet Singh Gulati, Ashish Gupta, Nagesh Chamarajnagar, Sandeep Seth Cardiothoracic Center, All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110029, India