Download
1 / 20
210 likes | 816 Views
Massive Transfusion in Trama. By R1 彭育仁. Brief History(1). 26 y/o male came to our ER due to massive bleeding from cutting wound over right neck and left head. Cons: irritable T/P/R:36.7/155/30, BP 120/59 mmHg

E N D
Massive Transfusion in Trama By R1 彭育仁
Brief History(1) • 26 y/o male came to our ER due to massive bleeding from cutting wound over right neck and left head. • Cons: irritable T/P/R:36.7/155/30, BP 120/59 mmHg Active bleeding was noted from cut r’t external and internal jugular vein and l’t temperal area.
Brief History (2) • Wound was pressured and IV catheters were set up using r’t femoral double lumen (12x12) and peripheral line with 20# catheter. After IV fluid replacement with L/R x 5 bottles and blood transfusion with whole blood 5 unit, he was sent to OR for surgical treatment.
Definition of massive transfusion(1) • The replacement of patient’s entire blood volume in a 24-hour period. • The transfusion of more than 20u of whole blood or 40u of PRBC. • The replacement of over 50% of circulating blood volume in 3 hour or less. • Loss of blood or more than 150ml/min
Definition of massive transfusion(2) • Massive transfusion is accompanied most frequently with significant blood loss or shock. • Although the volume of blood transfused may lead to a variety of potentially serious problems, the duration and severity of shock (hypoperfusion, acidosis, hypoxia) appears to be the primary derterminant of mortality and morbidity.
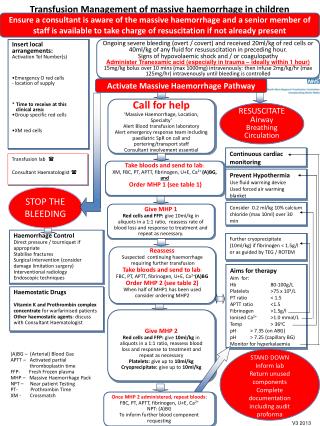
Initial Management(1) • Initual fluid resuscitation with colloid or crystalloid, which begins to replete intravascular volume. • Restoration of tissue oxygenation with RBC transfusion. • Primary surgical treatment of bleeding source to achieve hemostasis. • Replacement of hemostatic components diluted during massive transfusion.
Initial Management(2) • DO2 = CO x CaO2 = CO x {1.34 x Hb x SaO2 + 0.003 x PaO2} Initial fluid resuscitation can increase CO by Frank-Starling law. RBC transfusion can increase Hb.
Initial Fluid Resuscitation(1) • Crystalloid (N/S, L/R): * Most common fluid used due to cheaper and available. * Due to low colloid oncotic pressure, only 20% remain within IV space. Volume approximately 3 to 4 times of blood loss must be infused to maintain IV volume.
Initial Fluid Resuscitation(2) • Colloid: * Greater oncotic pressure and greater half life, so better volume expansion. * Less used due to cost and unavailability. * Large dose can impair hemostasis. * Which one is better has come into question.
Blood component • Whole blood: 250ml. containing PRBC 1u, FFP 1u and 30ml preservatives. • PRBC: ~100ml. Hct 70~80%. PRBC 1u can increase Hb 0.5 (Hct 1.5) • FFP: ~125ml. Containing coagulation factor, protein and plasma. • PLT: ~25ml. PLT 12u can increase PLT 60000.
Indications for blood transfusion • Whole blood: blood loss > 1500ml, better than PRBC + FFP. • PRBC: blood loss < 1000ml. • FFP: deficiency of coagulation factor and protein, massive transfusion. • PLT: thrombocytopenia, massive transfusion.
Emergency Transfusion • If blood type is known, an abbreviated cross match (<5min) can be done. • If blood type is not known, only PRBC of type O Rh (-) can be used, and further transfusions should be type O Rh (-) until anti-A and anti-B titers are determined in patient’s serum.
Role of Hb in blood transfusion • In young and healthy p’t, CO may increase enough to maintain adequate DO2 even Hb is 3g/dL if IV volume is sufficient. • In practice, Hb as low as 7 can be compensated by increasing CO. • Patient with known heart or lung disease should keep Hb > 10. • RBC transfusion decision should be made on a case-by-case basis according to ongoing blood loss, symptoms of impaired DO2 and signs of impending failure.
Monitoring patient • Vital signs are the most important indicator: HR, BP, RR, capillary perfusion time, Hb, estimated blood loss….etc. • More invasive monitor: CVP, A-line, U/O, pulmonary wedge pressure.
Anesthesia consideration(1) • Hypovolemia should be corrected prior to induction. • Rapid sequence for endotracheal intubation due to inadequate NPO and delayed gastric emptying. • Drugs should be choiced to minimize cardiovascular depression. • Administer small incremental dose to titrate effect.
Anesthesia consideration(2) • Hypnotics: Thiapental 0.3~1mg/kg, Midazolam 0.1~0.3mg/kg, Ketamine 1mg/kg, Etomidate 0.1~0.2mg/kg. • Muscle relaxant: SCC 1.5mg/kg, Rocuronium 1.2mg/kg. • Analgesics: Fentanyl 1-2ug/kg • Amnesia: Midazolam 1~2mg if not used for hypnotics.
Complications of blood transfusion(1) • Acute/chronic hemolytic reaction. • Infections. • Volume overload. • Transfusion-related acute lung injury. • GVHD. • Nonhemolytic febrile reaction. • Urticaria.
Complications of blood transfusion(2) • Hypothermia: Will induce arrhythmia. Warming all blood product is absolutely indicated. • Hypocalcemia (Citrate intoxication): Cardiac depression, aggravated by hepatic disease. • Hyperkalemia • Coagulopathy: Dilutional thrombocytopenia and decreased coagulation factor.
Factors Improving Survival • Survival following massive transfusion in past 10 years has significantly increased. • Factors associated with good outcome included aggressive correction of coagulopathy, more efficient use of warming measures, increased use of component therapy (blood bank available) and improved op skills.