Download
1 / 1
10 likes | 239 Views
Bruce H. Friedman & Michael M. Knepp Autonomic reactivity in high and low trait worry Procedure Three task sets: (1) Body position : orthostatic stress & supine rest (2) Active/passive stress : mental arithmetic & hand cold pressor (3) Imagery : relaxation & worry

E N D
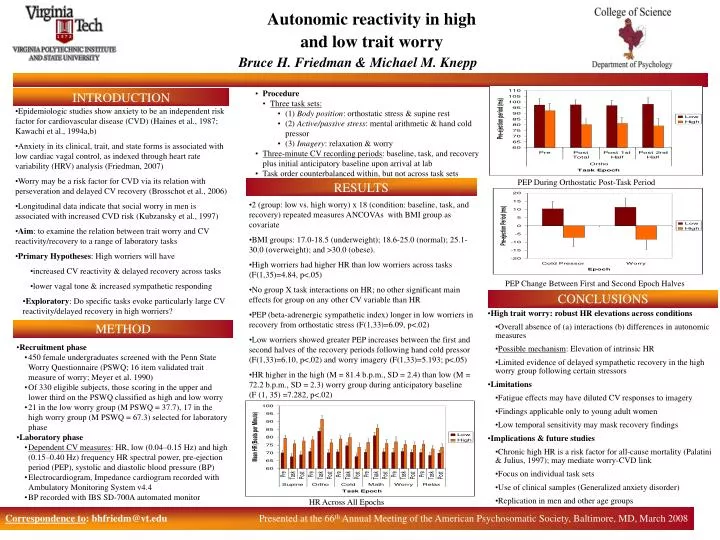
Bruce H. Friedman & Michael M. Knepp • Autonomic reactivity in high • and low trait worry • Procedure • Three task sets: • (1) Body position: orthostatic stress & supine rest • (2) Active/passive stress: mental arithmetic & hand cold pressor • (3) Imagery: relaxation & worry • Three-minute CV recording periods: baseline, task, and recovery plus initial anticipatory baseline upon arrival at lab • Task order counterbalanced within, but not across task sets INTRODUCTION • Epidemiologic studies show anxiety to be an independent risk factor for cardiovascular disease (CVD) (Haines et al., 1987; Kawachi et al., 1994a,b) • Anxiety in its clinical, trait, and state forms is associated with low cardiac vagal control, as indexed through heart rate variability (HRV) analysis (Friedman, 2007) • Worry may be a risk factor for CVD via its relation with perseveration and delayed CV recovery (Brosschot et al., 2006) • Longitudinal data indicate that social worry in men is associated with increased CVD risk (Kubzansky et al., 1997) • Aim: to examine the relation between trait worry and CV reactivity/recovery to a range of laboratory tasks • Primary Hypotheses: High worriers will have • increased CV reactivity & delayed recovery across tasks • lower vagal tone & increased sympathetic responding • Exploratory: Do specific tasks evoke particularly large CV reactivity/delayed recovery in high worriers? PEP During Orthostatic Post-Task Period RESULTS • 2 (group: low vs. high worry) x 18 (condition: baseline, task, and recovery) repeated measures ANCOVAs with BMI group as covariate • BMI groups: 17.0-18.5 (underweight); 18.6-25.0 (normal); 25.1-30.0 (overweight); and >30.0 (obese). • High worriers had higher HR than low worriers across tasks (F(1,35)=4.84, p<.05) • No group X task interactions on HR; no other significant main effects for group on any other CV variable than HR • PEP (beta-adrenergic sympathetic index) longer in low worriers in recovery from orthostatic stress (F(1,33)=6.09, p<.02) • Low worriers showed greater PEP increases between the first and second halves of the recovery periods following hand cold pressor (F(1,33)=6.10, p<.02) and worry imagery (F(1,33)=5.193; p<.05) • HR higher in the high (M = 81.4 b.p.m., SD = 2.4) than low (M = 72.2 b.p.m., SD = 2.3) worry group during anticipatory baseline (F (1, 35) =7.282, p<.02) PEP Change Between First and Second Epoch Halves CONCLUSIONS • High trait worry: robust HR elevations across conditions • Overall absence of (a) interactions (b) differences in autonomic measures • Possible mechanism: Elevation of intrinsic HR • Limited evidence of delayed sympathetic recovery in the high worry group following certain stressors • Limitations • Fatigue effects may have diluted CV responses to imagery • Findings applicable only to young adult women • Low temporal sensitivity may mask recovery findings • Implications & future studies • Chronic high HR is a risk factor for all-cause mortality (Palatini & Julius, 1997); may mediate worry-CVD link • Focus on individual task sets • Use of clinical samples (Generalized anxiety disorder) • Replication in men and other age groups METHOD • Recruitment phase • 450 female undergraduates screened with the Penn State Worry Questionnaire (PSWQ; 16 item validated trait measure of worry; Meyer et al. 1990) • Of 330 eligible subjects, those scoring in the upper and lower third on the PSWQ classified as high and low worry • 21 in the low worry group (M PSWQ = 37.7), 17 in the high worry group (M PSWQ = 67.3) selected for laboratory phase • Laboratory phase • Dependent CV measures: HR, low (0.04–0.15 Hz) and high (0.15–0.40 Hz) frequency HR spectral power, pre-ejection period (PEP), systolic and diastolic blood pressure (BP) • Electrocardiogram, Impedance cardiogram recorded with Ambulatory Monitoring System v4.4 • BP recorded with IBS SD-700A automated monitor • HR Across All Epochs Correspondence to: bhfriedm@vt.edu Presented at the 66th Annual Meeting of the American Psychosomatic Society, Baltimore, MD, March 2008






