Download
1 / 1
10 likes | 167 Views
SERIES OF CORNUAL PREGNANCY - PUTRAJAYA HOSPITAL EXPERIENCE Pavani.N , E.C.D’Silva, Hazim.W.A Department of Obstetrics & Gyneacology. Putrajaya Hospital. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE. Operative Procedures. Introduction.

E N D
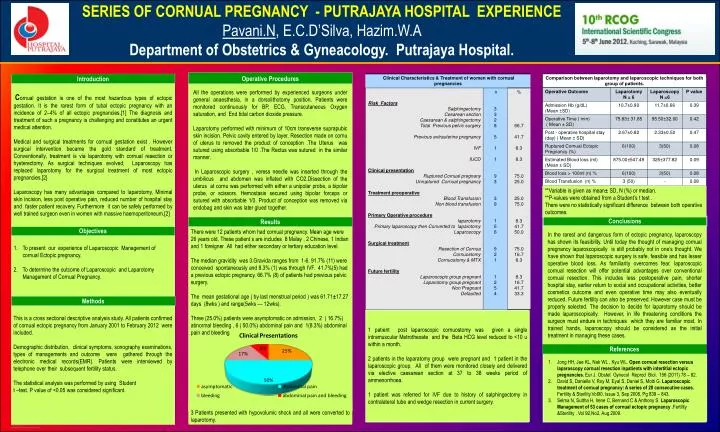
SERIES OF CORNUAL PREGNANCY - PUTRAJAYA HOSPITAL EXPERIENCE Pavani.N, E.C.D’Silva, Hazim.W.A Department of Obstetrics & Gyneacology. Putrajaya Hospital. OPTIONALLOGO HERE OPTIONALLOGO HERE OperativeProcedures Introduction Cornual gestation is one of the most hazardous types of ectopic gestation. It is the rarest form of tubal ectopic pregnancy with an incidence of 2–4% of all ectopic pregnancies.[1] The diagnosis and treatment of such a pregnancy is challenging and constitutes an urgent medical attention. Medical and surgical treatments for cornual gestation exist . However surgical intervention became the gold standard of treatment. Conventionally, treatment is via laparotomy with cornual resection or hysterectomy. As surgical techniques evolved; Laparoscopy has replaced laparotomy for the surgical treatment of most ectopic pregnancies.[2} Laparoscopy has many advantages compared to laparotomy, Minimal skin incision, less post operative pain, reduced number of hospital stay and faster patient recovery. Furthermore it can be safely performed by well trained surgeon even in women with massive haemoperitoneum.[2] All the operations were performed by experienced surgeons under general anaesthesia, in a dorsolithotomy position. Patients were monitored continuously for BP, ECG, Transcutaneous Oxygen saturation, and End tidal carbon dioxide pressure. Laparotomy performed with minimum of 10cm transverse suprapubic skin incision. Pelvic cavity entered by layer. Resection made on cornu of uterus to removed the product of conception .The Uterus was sutured using absorbable 1/0 .The Rectus was sutured in the similar manner. In Laparoscopic surgery , veress needle was inserted through the umbilicus and abdomen was inflated with CO2.Dissection of the uterus at cornu was performed with either a unipolar probe, a bipolar probe, or scissors. Hemostasis secured using bipolar forceps or sutured with absorbable 1/0. Product of conception was removed via endobag and skin was later glued together. **Variable is given as mean± SD, N (%) or median. **P-values were obtained from a Student’s t test . There were no statistically significant difference between both operative outcomes. Conclusions Results In the rarest and dangerous form of ectopic pregnancy, laparoscopy has shown its feasibility. Until today the thought of managing cornual pregnancy laparoscopically is still probably not in one’s thought. We have shown that laparoscopic surgery is safe, feasible and has lesser operative blood loss. As familiarity overcomes fear, laparoscopic cornual resection will offer potential advantages over conventional cornual resection. This includes less postoperative pain, shorter hospital stay, earlier return to social and occupational activities, better cosmetics outcome and even operative time may also eventually reduced. Future fertility can also be preserved. However case must be properly selected. The decision to decide for laparotomy should be made laparoscopically. However, in life threatening conditions the surgeon must endure in techniques which they are familiar most. In trained hands, laparoscopy should be considered as the initial treatment in managing these cases. Objectives There were 12 patients whom had cornual pregnancy. Mean age were 26 years old. These patient s are includes 8 Malay , 2 Chinese, 1 Indian and 1 foreigner .All had either secondary or tertiary education level. The median gravidity was 3.Gravida ranges from 1-6. 91.7% (11) were conceived spontaneously and 8.3% (1) was through IVF. 41.7%(5) had a previous ectopic pregnancy. 66.7% (8) of patients had previous pelvic surgery. The mean gestational age ( by last menstrual period ) was 61.71±17.27 days (8wks ) and range(5wks --- 12wks). Three (25.0%) patients were asymptomatic on admission, 2 ( 16.7%) abnormal bleeding , 6 ( 50.0%) abdominal pain and 1(8.3%) abdominal pain and bleeding • To present our experience of Laparoscopic Management of cornual Ectopic pregnancy. • To determine the outcome of Laparoscopic and Laparotomy Management of Cornual Pregnancy. Methods This is a cross sectional descriptive analysis study. All patients confirmed of cornual ectopic pregnancy from January 2001 to February 2012 were included. Demographic distribution, clinical symptoms, sonography examinations, types of managements and outcome were gathered through the electronic medical records(EMR). Patients were interviewed by telephone over their subsequent fertility status. The statistical analysis was performed by using Student t –test. P value of <0.05 was considered significant. 1 patient post laparoscopic cornuostomy was given a single intramuscular Metrothexate and the Beta HCG level reduced to <10 u within a month. 2 patients in the laparatomy group were pregnant and 1 patient in the laparoscopic group. All of them were monitored closely and delivered via elective caesarean section at 37 to 38 weeks period of ammenorrhoea. 1 patient was referred for IVF due to history of salphingectomy in contralateral tube and wedge resection in current surgery. References • Jong HH, Jae KL, Nak WL , Kyu WL. Open cornual resection versus laparoscopy cornual resection inpatients with intertitial ectopic pregnancies. Eur J. Obstet Gynecol Reprod Biol. 156 (2011) 78 – 82. • David S, Danielle V, Roy M, Eyal S, Daniel S, Motti G. Laparoscopic treatment of cornual pregnancy: A series of 20 consecutive cases. Fertility & Sterility.Vol90, Issue 3, Sep 2008, Pg 839 – 843. • Selma N, Suttha H, Irene C, Bernand C & Anthony S. Laparoscopic Management of 53 cases of cornual ectopic pregnancy .Fertility &Sterility . Vol 92,No2, Aug 2009. 3 Patients presented with hypovolumic shock and all were converted to laparotomy.






