Download
1 / 1
10 likes | 342 Views
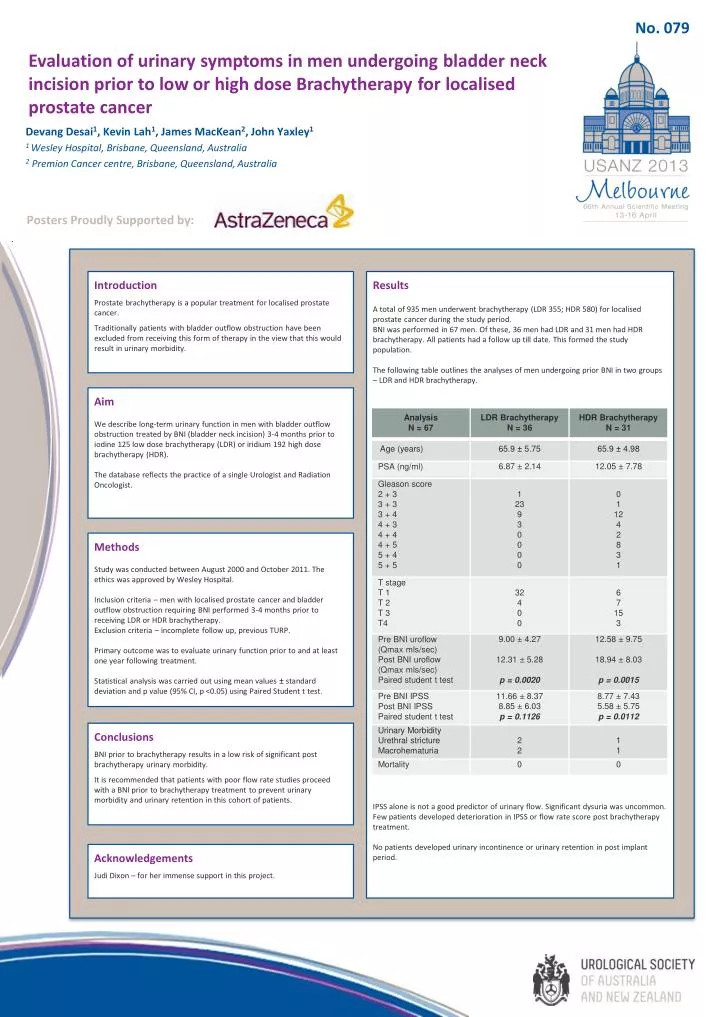
No. 079. Evaluation of urinary symptoms in men undergoing bladder neck incision prior to low or high dose Brachytherapy for localised prostate cancer. Devang Desai 1 , Kevin Lah 1 , James MacKean 2 , John Yaxley 1 1 Wesley Hospital, Brisbane, Queensland, Australia

E N D
No. 079 Evaluation of urinary symptoms in men undergoing bladder neck incision prior to low or high dose Brachytherapy for localisedprostate cancer Devang Desai1, Kevin Lah1, James MacKean2, John Yaxley1 1 Wesley Hospital, Brisbane, Queensland, Australia 2Premion Cancer centre, Brisbane, Queensland, Australia Posters Proudly Supported by: Introduction Prostate brachytherapy is a popular treatment for localised prostate cancer. Traditionally patients with bladder outflow obstruction have been excluded from receiving this form of therapy in the view that this would result in urinary morbidity. Results A total of 935 men underwent brachytherapy (LDR 355; HDR 580) for localised prostate cancer during the study period. BNI was performed in 67 men. Of these, 36 men had LDR and 31 men had HDR brachytherapy. All patients had a follow up till date. This formed the study population. The following table outlines the analyses of men undergoing prior BNI in two groups – LDR and HDR brachytherapy. IPSS alone is not a good predictor of urinary flow. Significant dysuria was uncommon. Few patients developed deterioration in IPSS or flow rate score post brachytherapy treatment. No patients developed urinary incontinence or urinary retention in post implant period. Aim We describe long-term urinary function in men with bladder outflow obstruction treated by BNI (bladder neck incision) 3-4 months prior to iodine 125 low dose brachytherapy (LDR) or iridium 192 high dose brachytherapy (HDR). The database reflects the practice of a single Urologist and Radiation Oncologist. Methods Study was conducted between August 2000 and October 2011. The ethics was approved by Wesley Hospital. Inclusion criteria – men with localised prostate cancer and bladder outflow obstruction requiring BNI performed 3-4 months prior to receiving LDR or HDR brachytherapy. Exclusion criteria – incomplete follow up, previous TURP. Primary outcome was to evaluate urinary function prior to and at least one year following treatment. Statistical analysis was carried out using mean values ± standard deviation and p value (95% CI, p <0.05) using Paired Student t test. Conclusions BNI prior to brachytherapy results in a low risk of significant post brachytherapy urinary morbidity. It is recommended that patients with poor flow rate studies proceed with a BNI prior to brachytherapy treatment to prevent urinary morbidity and urinary retention in this cohort of patients. Acknowledgements Judi Dixon – for her immense support in this project.