Download
1 / 25
250 likes | 408 Views
Protein-, Mineral- & Fluid-Modified Diets for Kidney Diseases. Chapter 23. Roles of Kidneys. Filtration of blood & removal of excess fluid & wastes for elimination in urine Regulation of fluid volume & osmolarity, electrolyte concentration & acid-base balance

E N D
Protein-, Mineral- & Fluid-Modified Diets for Kidney Diseases Chapter 23 Nutrition & Diet Therapy, 7th Edition
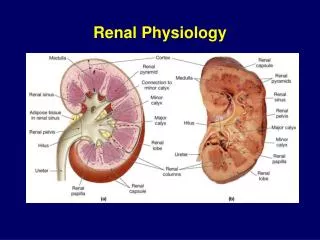
Roles of Kidneys • Filtration of blood & removal of excess fluid & wastes for elimination in urine • Regulation of fluid volume & osmolarity, electrolyte concentration & acid-base balance • Excretion of metabolic wastes, drugs & toxins • Secretion of enzyme renin to regulate blood pressure • Production of hormone erythropoietin to stimulate production of RBCs • Conversion of vitamin D to active form, helping to maintain bone tissue Nutrition & Diet Therapy, 7th Edition
Not a specific disease—kidney disorders that result in urinary protein losses in excess of 3 grams/day Occurs most often in children between 1 ½-4 years old Damage to glomeruli increases permeability to plasma proteins, allowing protein to escape into the urine Can progress to renal failure Causes Infection Chemical damage Immunological & hereditary disorders Diabetes mellitus Other disorders involving glomerulus Clinical findings Proteinuria Low serum albumin levels Edema Elevated blood lipids Blood coagulation disorders I. Nephrotic Syndrome Nutrition & Diet Therapy, 7th Edition
Treatment goals: include relief of symptoms & prevention of kidney damage Drugs Anti-inflammatory drugs (usually corticosteroids) ACE inhibitors Diuretics Antihypertensives Immunosuppressants Lipid-lowering medications Nutrition Meet protein (.8-1g/Kg)& energy (35 kcal/Kg)needs to minimize muscle tissue loss Low sat fats, cholesterol Low refined sugars Sodium restriction(1-2g/d) Potassium-rich foods (if potassium-wasting diuretics are used) Vitamin & mineral supplements Nephrotic Syndrome Nutrition & Diet Therapy, 7th Edition
II. Acute Renal Failure • Rapid deterioration of kidney function • Reduction of urinary output • Accumulation of nitrogenous wastes in blood • Degree of renal dysfunction varies from mild to severe • Causes • Can result from number of disorders • Often develops as consequence of severe illness, infections, injury or surgery • Causes usually classified as prerenal, intrarenal or postrenal Nutrition & Diet Therapy, 7th Edition
Consequences Fluid & electrolyte imbalance Oliguria: production of <400 mL urine/day Hyperkalemia: elevated serum potassium levels Hyperphosphatemia: elevated serum phosphate levels Uremia Accumulation of nitrogen-containing waste products in blood Blood urea nitrogen (BUN) Creatinine Uric acid Treatment Drug therapy Diuretics Correction of hyperkalemia Nutrition Meet protein (.6-.8g/Kg)& energy (35kcal/Kg) needs Restoration of fluid balance (urine+500ml) Replacement of electrolytes (2-3g Na/d, K & P restricted) Enteral & parenteral nutrition (hcal, ipro and electrolytes) Renal dialysis Acute Renal Failure Nutrition & Diet Therapy, 7th Edition
III.Chronic Renal Failure • Characterized by gradual & irreversible deterioration in kidney function; may follow acute renal failure • Causes • Diabetes mellitus (about 43% of cases) • Hypertension (about 26% of cases) • Inflammatory, immunological or hereditary diseases that directly affect kidneys • End-stage renal disease (ESRD): advanced stage of chronic renal failure in which dialysis or kidney transplant is necessary to sustain life Nutrition & Diet Therapy, 7th Edition
Early Stages Anorexia Fatigue Headache Hypertension Itching Kidney inflammation or nephrotic syndrome Nausea & vomiting Proteinuria, hematuria Advanced Stages Anemia, bleeding tendency Cardiovascular disease Confusion, mental impairment Electrolyte abnormalities Fluid retention Metabolic acidosis Peripheral neuropathy Protein-energy malnutrition Reduced immunity Renal osteodystrophy Chronic Renal Failure Consequences Nutrition & Diet Therapy, 7th Edition
Chronic Renal Failure • Uremic syndrome • Cluster of symptoms & complications that develops during final stages of chronic renal failure • GFR (rate of kidneys form filtrate)<15 mL/minute • BUN exceeds 60 mg/dL • Anemia • Bone disease • Hormonal imbalance • Bleeding impairment • Increased risk of cardiovascular disease • Reduced immunity Nutrition & Diet Therapy, 7th Edition
Treatment goals: slow disease progression & prevent or alleviate symptoms Drug therapy Antihypertensives Erythropoetin Phosphate binders(iP) Na bicarbonate(iacidosis) Cholesterol-lowering drugs Vitamin D supplementation(hCa) Dialysis Hemodialysis Peritoneal dialysis Nutrition Energy intake to maintain healthy weight & prevent wasting Low-protein (unless dialysis), low sat fat Regulation of fluid & sodium intakes based on total urine output, changes in body weight, blood pressure & serum sodium levels Regulation of potassium intake based on potassium levels & use of diuretics Vitamin & mineral supplementation Enteral & parenteral nutrition Chronic Renal Failure Nutrition & Diet Therapy, 7th Edition
Kidney transplants Preferred alternative to dialysis in ESRD Restores kidney function Allows more liberal diet Frees patient from routine dialysis Barriers to transplantation Supply of suitable kidneys vs. demand (<20% are recipients) Patient-related barriers: age, financial difficulties, abnormalities of urinary tract Immunosuppressive drug therapy Used to prevent tissue rejection Include side effects that alter nutrition status (FDI) Nutrition Increased E & protein requirements after surgery Control of hyperglycemia, blood lipids, electrolyte balances, calcium levels Avoidance of foods that can cause food-borne illnesses Chronic Renal Failure Nutrition & Diet Therapy, 7th Edition
IV. Kidney Stones • Crystalline mass that forms within urinary tract • May be asymptomatic or may cause severe pain or blockage of urinary tract as the stone passes • Tend to recur, but can be prevented with diet & medical treatment • Formation of kidney stones • Develop when stone constituents become concentrated in urine • Allows formation & growth of crystals • Composed of calcium oxalate (75%) or uric acid, amino acid cystine, magnesium ammonium phosphate • Formation promoted by factors that reduce urine volume, block urine flow or increase concentrations of stone-forming substances Nutrition & Diet Therapy, 7th Edition
Calcium oxalate stones Usually associated with hypercalciuria Results from excessive or impaired calcium reabsorption, elevated levels of parathyroid hormone or vitamin D Reduction of dietary intake of oxalate recommended Uric acid stones Develop in highly acidic urine or in presence of high amounts of uric acid or both Frequently associated with gout Diet rich in purines also contributes Kidney Stones Nutrition & Diet Therapy, 7th Edition
Kidney Stones • Consequences • Renal colic • Hematuria • Urinary tract complications • Prevention & treatment • Increased fluid intake of 12-16 cups daily • Water, tea, coffee, wine, beer acceptable • Avoid apple & grapefruit juices(h risk) • Diet & drugs to reduce urinary calcium & oxalate levels, uric acid levels • Adjustment in calcium (moderate), oxalate (i levels), moderate protein & sodium intakes, ?purine restriction for uric acid stones Nutrition & Diet Therapy, 7th Edition
Nutrition in Practice—Dialysis • Dialysis offers life-sustaining treatment for chronic renal failure • Permanent treatment or temporary measure • Can restore fluid & electrolyte balances • Removes excess fluids & wastes through processes of diffusion, osmosis & ultrafiltration • Hemodialysis • Peritoneal dialysis Nutrition & Diet Therapy, 7th Edition
Nutrition in Practice—Dialysis • Dialysate (solution similar in composition to normal blood plasma) delivered to compartment beside semi-permeable membrane • Blood flows along other side of membrane • Concentrations of dialysate & blood affect movement of solutes across the semi-permeable membrane • Semi-permeable membrane acts as filter • Small molecules (i.e. urea & glucose) can pass through membrane pores • Large molecules are unable to cross Nutrition & Diet Therapy, 7th Edition
Nutrition in Practice—Dialysis • Hemodialysis • Dialyzer used to cleanse blood • Treatments usually require 3-4 hours, at least 3 times per week • Most patients receive treatment in dialysis centers; some (about 2%) are treated at home • Complications • Infection & blood clotting at vascular access site • Hypotension • Muscle cramping • Blood losses, worsening anemia • Other: headaches, weakness, n&v, agitation Nutrition & Diet Therapy, 7th Edition
Nutrition in Practice—Dialysis • Peritoneal dialysis • Peritoneal membrane surrounding abdominal organs serves as the semi-permeable membrane • Dialysate infused through catheter into peritoneal space (4-6 hrs) • Dialysate solution drained & exchanged (avg.4x/d, 30min.) • Advantage over hemodialysis: vascular access not required, fewer dietary restrictions • Complications • Infection (peritonitis) • Blood clotting in catheter, catheter migration • Abdominal hernia Nutrition & Diet Therapy, 7th Edition