Download
1 / 1
10 likes | 111 Views
Interactive Visualization of Time-Resolved Contrast-Enhanced Magnetic Resonance Angiography (CE-MRA) Ethan Brodsky 1 and Walter F. Block 2,3 Departments of Electrical Engineering 1 , Biomedical Engineering 2 , and Medical Physics 3 University of Wisconsin-Madison.

E N D
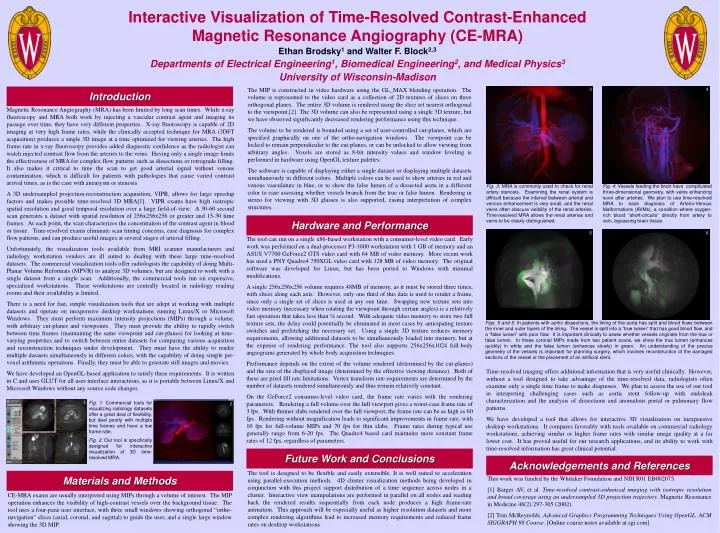
Interactive Visualization of Time-Resolved Contrast-Enhanced Magnetic Resonance Angiography (CE-MRA) Ethan Brodsky1 and Walter F. Block2,3 Departments of Electrical Engineering1, Biomedical Engineering2, and Medical Physics3 University of Wisconsin-Madison The MIP is constructed in video hardware using the GL_MAX blending operation. The volume is represented to the video card as a collection of 2D textures of slices on three orthogonal planes. The entire 3D volume is rendered using the slice set nearest orthogonal to the viewpoint.[2] The 3D volume can also be represented using a single 3D texture, but we have observed significantly decreased rendering performance using this technique. The volume to be rendered is bounded using a set of user-controlled cut-planes, which are specified graphically on one of the ortho-navigation windows. The viewpoint can be locked to remain perpendicular to the cut-planes, or can be unlocked to allow viewing from arbitrary angles. Voxels are stored as 8-bit intensity values and window leveling is performed in hardware using OpenGL texture palettes. The software is capable of displaying either a single dataset or displaying multiple datasets simultaneously in different colors. Multiple colors can be used to show arteries in red and venous vasculature in blue, or to show the false lumen of a dissected aorta in a different color to ease assessing whether vessels branch from the true or false lumen. Rendering in stereo for viewing with 3D glasses is also supported, easing interpretation of complex structures. Introduction 3 4 Magnetic Resonance Angiography (MRA) has been limited by long scan times. While x-ray fluoroscopy and MRA both work by injecting a vascular contrast agent and imaging its passage over time, they have very different properties. X-ray fluoroscopy is capable of 2D imaging at very high frame rates, while the clinically accepted technique for MRA (3DFT acquisition) produces a single 3D image at a time optimized for viewing arteries. The high frame rate in x-ray fluoroscopy provides added diagnostic confidence as the radiologist can watch injected contrast flow from the arteries to the veins. Having only a single image limits the effectiveness of MRA for complex flow patterns such as dissections or retrograde filling. It also makes it critical to time the scan to get good arterial signal without venous contamination, which is difficult for patients with pathologies that cause varied contrast arrival times, as is the case with aneurysm or stenosis. A 3D undersampled projection-reconstruction acquisition, VIPR, allows for large speedup factors and makes possible time-resolved 3D MRA[1]. VIPR exams have high isotropic spatial resolution and good temporal resolution over a large field-of-view. A 30-60 second scan generates a dataset with spatial resolution of 256x256x256 or greater and 15-30 time frames. At each point, the scan characterizes the concentration of the contrast agent in blood or tissue. Time-resolved exams eliminate scan timing concerns, ease diagnosis for complex flow patterns, and can produce useful images at several stages of arterial filling. Unfortunately, the visualization tools available from MRI scanner manufacturers and radiology workstation vendors are ill suited to dealing with these large time-resolved datasets. The commercial visualization tools offer radiologists the capability of doing Multi-Planar Volume Reformats (MPVR) to analyze 3D volumes, but are designed to work with a single dataset from a single scan. Additionally, the commercial tools run on expensive, specialized workstations. These workstations are centrally located in radiology reading rooms and their availability is limited. There is a need for fast, simple visualization tools that are adept at working with multiple datasets and operate on inexpensive desktop workstations running Linux/X or Microsoft Windows. They must perform maximum intensity projections (MIPs) through a volume, with arbitrary cut-planes and viewpoints. They must provide the ability to rapidly switch between time frames (maintaining the same viewpoint and cut-planes) for looking at time-varying properties and to switch between entire datasets for comparing various acquisition and reconstruction techniques under development. They must have the ability to render multiple datasets simultaneously in different colors, with the capability of doing simple per-voxel arithmetic operations. Finally, they must be able to generate still images and movies. We have developed an OpenGL-based application to satisfy these requirements. It is written in C and uses GLUT for all user-interface interactions, so it is portable between Linux/X and Microsoft Windows without any source code changes. Fig. 3: MRA is commonly used to check for renal artery stenosis. Examining the renal system is difficult because the interval between arterial and venous enhancement is very small, and the renal veins often obscure visibility of the renal arteries. Time-resolved MRA allows the renal arteries and veins to be clearly distinguished. Fig. 4: Vessels feeding the brain have complicated three-dimensional geometry, with veins enhancing soon after arteries. We plan to use time-resolved MRA to ease diagnosis of Arterio-Venous Malformations (AVMs), a condition where oxygen-rich blood “short-circuits” directly from artery to vein, bypassing brain tissue. Hardware and Performance 5 6 The tool can run on a single x86-based workstation with a consumer-level video card. Early work was performed on a dual-processor P3-1000 workstation with 1 GB of memory and an ASUS V7700 GeForce2 GTS video card with 64 MB of video memory. More recent work has used a PNY Quadro4 750XGL video card with 128 MB of video memory. The original software was developed for Linux, but has been ported to Windows with minimal modifications. A single 256x256x256 volume requires 48MB of memory, as it must be stored three times, with slices along each axis. However, only one third of this data is used to render a frame, since only a single set of slices is used at any one time. Swapping new texture sets into video memory (necessary when rotating the viewpoint through certain angles) is a relatively fast operation that takes less than ¼ second. With adequate video memory to store two full texture sets, the delay could potentially be eliminated in most cases by anticipating texture switches and prefetching the necessary set. Using a single 3D texture reduces memory requirements, allowing additional datasets to be simultaneously loaded into memory, but at the expense of rendering performance. The tool also supports 256x256x1024 full-body angiograms generated by whole body acquisition techniques. Performance depends on the extent of the volume rendered (determined by the cut-planes) and the size of the displayed image (determined by the effective viewing distance). Both of these are pixel fill rate limitations. Vertex transform rate requirements are determined by the number of datasets rendered simultaneously and thus remain relatively constant. On the GeForce2 consumer-level video card, the frame rate varies with the rendering parameters. Rendering a full volume over the full viewport gives a worst-case frame rate of 3 fps. With thinner slabs rendered over the full viewport, the frame rate can be as high as 60 fps. Rendering without magnification leads to significant improvements in frame rate, with 10 fps for full-volume MIPs and 70 fps for thin slabs. Frame rates during typical use generally range from 6-20 fps. The Quadro4 based card maintains more constant frame rates of 12 fps, regardless of parameters. Figs. 5 and 6: In patients with aortic dissections, the lining of the aorta has split and blood flows between the inner and outer layers of the lining. The vessel is split into a “true lumen” that has good blood flow, and a “false lumen” with poor flow. It is important clinically to asses whether vessels originate from the true or false lumen. In these coronal MIPs made from two patient scans, we show the true lumen (enhances quickly) in white and the false lumen (enhances slowly) in green. An understanding of the precise geometry of the vessels is important for planning surgery, which involves reconstruction of the damaged sections of the vessel or the placement of an artificial stent. Time-resolved imaging offers additional information that is very useful clinically. However, without a tool designed to take advantage of the time-resolved data, radiologists often examine only a single time frame to make diagnoses. We plan to assess the use of our tool in interpreting challenging cases such as aortic stent follow-up with endoleak characterization and the analysis of dissections and anomalous portal or pulmonary flow patterns. We have developed a tool that allows for interactive 3D visualization on inexpensive desktop workstations. It compares favorably with tools available on commercial radiology workstations, achieving similar or higher frame rates with similar image quality at a far lower cost. It has proved useful for our research applications, and its ability to work with time-resolved information has great clinical potential. 1 Fig. 1: Commercial tools for visualizing radiology datasets offer a great deal of flexibility, but deal poorly with multiple time frames and have a low frame rate. Fig. 2: Our tool is specifically designed for interactive visualization of 3D time-resolved MRA. 2 Future Work and Conclusions Acknowledgements and References The tool is designed to be flexible and easily extensible. It is well suited to acceleration using parallel-execution methods. 4D cluster visualization methods being developed in conjunction with this project support distribution of a time sequence across nodes in a cluster. Interactive view manipulations are performed in parallel on all nodes and reading back the rendered results sequentially from each node produces a high frame-rate animation. This approach will be especially useful as higher resolution datasets and more complex rendering algorithms lead to increased memory requirements and reduced frame rates on desktop workstations. Materials and Methods This work was funded by the Whitaker Foundation and NIH R01 EB002075. [1] Barger AV, et al. Time-resolved contrast-enhanced imaging with isotropic resolution and broad coverage using an undersampled 3D projection trajectory. Magnetic Resonance in Medicine 48(2):297-305 (2002). [2] Tom McReynolds. Advanced Graphics Programming Techniques Using OpenGL. ACM SIGGRAPH 98 Course. [Online course notes available at sgi.com] CE-MRA exams are usually interpreted using MIPs through a volume of interest. The MIP operation enhances the visibility of high-contrast vessels over the background tissue. The tool uses a four-pane user interface, with three small windows showing orthogonal “ortho-navigation” slices (axial, coronal, and sagittal) to guide the user, and a single large window showing the 3D MIP.






