Download
1 / 67
820 likes | 1.38k Views
Quality Improvement in Pediatric Practice. David Gremse, MD, FAAP, FACG Professor and Chair of Pediatrics University of Nevada School of Medicine. Quality Improvement is a formal approach to the analysis and performance and ways to improve it. Commonly used QI models include:

E N D
Quality Improvement inPediatric Practice David Gremse, MD, FAAP, FACG Professor and Chair of Pediatrics University of Nevada School of Medicine
Quality Improvement is a formal approach to the analysis and performance and ways to improve it. • Commonly used QI models include: • FADE (Focus, Analyze, Develop, Execute) • PDSA (Plan, Do, Study, Act) • Six Sigma • CQI – Continuous Quality Improvement • TQM – Total Quality Management What is QI?
Quality Assurance – QA is reactive, retrospective, policing. Often involves finding who was at fault when something goes wrong • Quality Improvement – QI can be retrospective or prospective. The aim is improvement by measuring where things are and how to make them better. It avoids placing blame and creates systems to reduce errors. Quality Assurance vs. Quality Improvement
Which staff member failed to transfer the call to the correct extension? • How do we reduce errors in collecting contact information? • Who was at fault for the patients bad outcome, the physicians or the nurses? • How could we increase the efficiency of chart filing? QA vs. QI
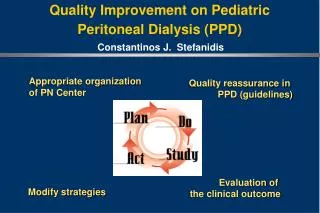
Plan – plan a change or test how something works • Do – Carry out the plan • Study – Look at the results. What did you find out? • Act – Decide what actions should be taken to improve PDSA Cycles
Model for Improvementask 3 important questions to identify the "what" in changing your practice. • PDSA Cycleuses the 4 steps for testing and implementation: Plan, Do, Study, and Act. Apply these 4 steps of change in practice. • Cycles of Improvementuses the PDSA process in practice. Continue refining improvements and spread successful changes throughout the practice. Action Plans
The Model for Improvement is an approach to: • planning, testing, and implementing improvements in clinical processes and systems of care. • It can be used in health care and non-health care settings to provide an action-oriented approach to putting new ideas into practice. Model for Improvement
A gap exists between current performance and desired performance. • Before you change anything, ask yourself 3 fundamental questions: • AIM: What are we trying to accomplish? • MEASURES: How will we know that a change is an improvement? • IDEAS: What change can we make that will result in an improvement? Why Change?
PLAN- Make a "blueprint" for what you will change, predicting the results of the test, specifying the steps you will take, identifying who will be responsible for what, and determining which patients will be involved. • DO- Try your change with a few patients or for a short time. • STUDY- Check to see if you made the changes you planned and if they resulted in an improvement. Do this by comparing the results with the prediction. • ACT- Based on the results of the study phase, decide how to increase the scope if the results were positive or refine or plan another test if the results were less than desirable PDSA Cycles
When you have a number of ideas or changes ready to test, the PDSA cycle, a quality improvement model developed by W.E. Demingprovides a systematic approach, or process, for planning, executing, studying, and implementing changes. PDSA Cycles
Works best when done on a small scale. • This helps to maximize the impact from a small change and refine ideas before expanding on a larger scale. • When planning PDSA cycles, consider trying things with 1 or 2 patients or 1 or 2 staff members for a couple days. • Plan multiple tests that can occur simultaneously and rapidly to accelerate your learning. • By starting small and testing quickly, you can rapidly test an idea and then expand it in the next testing cycle or series of cycles. PDSA Cycles
Oswego Pediatrics, located in Oswego, NY, on the banks of Lake Ontario, has a population of about 17,500. • It serves children from Oswego and surrounding counties along with 2 other pediatric practices and 2 family medicine practices. • The patient population is about 95% white, representing a range of family resources and types of insurance, including about 20% low-income families Action Plan Case Study
The practice has 3 full-time and 2 part-time pediatricians and 1 full-time nurse practitioner. • Each provider usually sees between 24 and 35 patients a day, depending on the season, with well-child visits evenly distributed throughout the morning and a few well-child visits in the afternoons owing to same-day appointments for sick children. • The staff includes 1 RN, 2 LPNs, 1 medical assistant, and 5 administrative personnel for scheduling and billing. • They share a professional office building with an accountant, a physical therapist, and a counseling service. Action Plan Case Study
Dr Saunders, who has been with the practice for 5 years, is concerned about the trends in childhood overweight and that the practice does not have an approach to identify children who are overweight or at risk for being overweight. • Although the practice has always provided support for optimal nutrition in the first year of life with a standard set of handouts for each well-baby visit, there are no resources to help families with older children. Action Plan Case Study
The practice calculates and plots BMI at well-child visits. • The MA measures height and weight and plots each on the appropriate growth curve, but providers calculate and plot BMI. • Forms are kept in the provider work area and added to the chart after the visits. • One pediatrician uses an iPhone app, one a pocket chart, and the rest use BMI wheels located in drawers at the nurses' station or in the provider's work area. Action Plan Case Study
Dr Saunders is willing to take the lead in her practice to develop a more systematic approach to address the problem of childhood obesity-but where does she start? Action Plan Case Study
3 Questions – Ask AIM • AIM: What are we trying to accomplish? • IDEAS: What change can we make that will result in an improvement? • MEASURES: How will we know that a change is an improvement? Why Change?
Oswego Pediatrics is ready to plan its first improvement change for the aim it established: • AIM STATEMENT: "Oswego Pediatrics will assess all patients' nutritional status through routine measurement of BMI and will support family behaviors to achieve optimal nutritional status though regular counseling, goal setting, and appropriate follow-up of children with less than satisfactory nutritional status.” Case Study: Oswego Peds
GAP: "BMI is not routinely calculated and documented on patient charts.” • The team met with front-desk staff members to ask them about placing BMI charts on the front of all patient charts for children being seen for well-child visits or sports physicals. • The front-desk staff expressed concern about the number of items they already need to compile, so a PDSA cycle is planned to see if this new idea can be incorporated into the flow. Case Study: Oswego Peds
GOAL: "BMI forms will be placed on the front of all charts of children 2 years or older being seen for well-child visits or sports physicals.” • They want to determine if this change could be incorporated easily into the current front-desk flow for well-child visits without excess stress on the front-desk staff. Case Study: Oswego Peds
Copies of BMI forms are placed in a folder next to well-child visit forms in the front filing cabinet. • When a patient checks in, the front-desk staff member checks the chart to see if a BMI form is already started. If not, he or she will put a BMI form and the usual well-child visit form on the front of the chart. • A note reading "REMEMBER BMI FORM" is placed on the cabinet where the forms are kept. • Nurses track how often the forms are placed correctly on patient charts and observe how the front-desk staff adapts to the additional step. Case Study: PLAN
The team tries this on a Tuesday morning when 3 providers are working and 5 well-child visits and 1 sports physical for children 2 years or older are scheduled. Case Study: DO
The nurses note that check-in did not take longer, the front-desk staff did not seem frustrated or upset, and the BMI forms were with the well-child visit forms on the chart 5 of 6 times. • However, in 2 of these cases, the form for the wrong sex was attached to the chart, requiring the nurse to return to the front-desk to obtain the correct form. Case Study: STUDY
The nurses decide to keep a supply of forms in their work area in case the mix-up happens again, but they also discussed the issue with the front-desk staff. • For the next test, they decide to place the forms in color-coded files (blue for boys, red for girls) to see if this helps improve the accuracy of selecting the correct form. Case Study: ACT
What are we testing? • Whom are we testing the change on? • When are we testing? • Where are we testing? • Who will implement the cycle? • What tools are needed • What is our measurement plan? • What barriers exist? • What do we expect to happen? Developing an Action Plan
Make a prediction about the expected outcome to help assess whether the cycle is a success. • If you can answer the preceding questions, you are probably done planning! • Build on your existing approach during this test. What examples of successful patient education and communication exist within your office that can you learn from? Developing an Action Plan
Plan a change that addresses a performance gap within your own practice. Use the Improvement Planning Worksheet. • The planning activity has 3 parts: • 1.Write an effective aim for your practice. • 2.Select a performance gap in your practice. • 3.Generate ideas about changes you could make in your practice to accomplish your aim. Developing an Action Plan
The first part of this activity is to write an effective aim statement for your practice. • Remember, an aim statement describes what you are trying to accomplish in your improvement efforts. It articulates the results you hope to see because of the changes you make. • It should be clear, numeric, focused, flexible, and a stretch. It should include: Writing an Aim Statement
It should be clear, numeric, focused, flexible, and a stretch. It should include: 1.A description of the desired improvement 2.The specific patient population to whom the change will apply 3.Guidance for carrying out the work Writing an Aim Statement
"We aim to assess all patients' nutritional status through routine measurement of BMI and to support family behaviors to achieve optimal nutritional status though regular counseling, goal setting, and appropriate follow-up of children with less than satisfactory nutritional status." Aim Statement Example
Every aim requires multiple small tests of change. The second part of this activity is to select a performance gap that, if closed, will move you closer to your aim. A performance gap is a discrepancy between actual and desired performance • Example: BMI is not routinely calculated and documented on patient charts. A goal might be 95% in calculating and charting BMI for patients, ages 2 - 18 years, at every patient visit. Select an Area to Change
Closing Performance Gaps What performance gaps have you identified in the nutritional care your practice provides? For your first improvement effort, it is recommended that you choose an area to change that has high impact but will be easy to implement. Consider these questions: 1. How many patients will it affect? 2. What is the frequency of the problem? 3. What barriers need to be overcome?
Plot height, weight, and BMI in chart. • For this performance gap, an appropriate goal or measure of success is: • For 95% of patients, height, weight and BMI will be plotted for each visit. Performance Goals:Plot BMI
For this performance gap, an appropriate goal or measure of success is: • For 95% of children, nutritional status will be documented at every visit. Performance Goals:Document Nutritional Status
For this performance gap, an appropriate goal or measure of success is: • For 95% of patients and families, discussion of nutritional status will be documented at every visit. Performance Goals:Discuss Nutritional Status
For this performance gap, an appropriate goal or measure of success is: • For 95% of patients whose nutritional status is not satisfactory, the chart will indicate an estimate of caloric intake. Performance Goals:Estimate Caloric Intake
For this performance gap, an appropriate goal or measure of success is: • For 95% of patients whose nutritional status is not satisfactory, the chart will indicate a plan to increase or decrease caloric intake. Performance Goals:Order Caloric Intake Plan
For 95% of patients whose nutritional status is not satisfactory and whose disease may lead to increased requirements, the chart will indicate a plan to evaluate for increased disease activity or to intensify disease therapy. Performance Goals:Document Treatment Plan
For this performance gap, an appropriate goal or measure of success is: • For 95% of patients with unsatisfactory nutritional status, a follow-up appointment will be made. Performance Goals:Document Follow Up
The third part of this activity is to generate ideas for change that could help you meet your goal and bring you closer to your aim. For the performance gap and goal you selected, here are some ideas you may want to consider as you plan your first change: Ideas for PDSA Cycles
Discuss follow-up schedule with practice team. Set concrete rules for frequency of follow-up visits. Use an algorithm or pathway to reinforce the need for follow-up appointments. • Determine appropriate billing codes for follow-up visits. • Develop a more efficient schedule that will allow for more follow-up appointments. You can do this by working to decrease no-show appointments. Ideas for PDSA Cycles
Discuss with family expectations for follow-up. Schedule next follow-up visit before checkout. • During evaluation visits, set expectations with child and family about the importance of follow-up to assess effectiveness of therapy, monitor response, and adjust treatment as necessary. • Place reminder calls to families before scheduled appointment. Ideas for PDSA Cycles
Remember, ideas can come from things you’ve read, brainstorming with others, or flowcharting your current process. Review the Nutrition Performance Gaps worksheet, which shows the relationships between performance gaps, goals, barriers, and ideas for change. • Once you have generated some ideas, select one of them for your first test. Then, develop a specific plan for the test. • Who will do the test? • What will they do? • Which patients will be involved? • When, where, and how will you conduct the test? • What tools will you need? • How you will track your progress? Ideas for PDSA Cycles
Generate at least 3 ideas for change that could help you accomplish your aim statement. • Select an idea for your 1st test and record it on a worksheet. • Consider any barriers you would have to overcome in your practice to achieve your performance goal and record them on your worksheet. • Formulate a specific plan to test your idea. List the tasks & tools needed to perform the test. Also predict what will happen when the test is carried out. Ideas for PDSA Cycles
In the second step of the PDSA cycle, you will do, or carry out the test. • This involves setting a date, developing any needed tools, and training people who will participate in the test. • Remember to try your change with a few patients over a short period of time. • The question the test must answer is: Did we accomplish what we had hoped? Ideas for PDSA Cycles: Do Stage
Test your idea in practice by trying a change with a few patients over a short period of time. Collect data that can be measured so you can document what happened because of the change. • Describe what happened when you ran the test on your worksheet. • With your team, discuss how the change affected practice. Share personal observations and analysis and solicit input from others. Ideas for PDSA Cycles: Do Stage
After planning and doing your test, the third step in the PDSA cycle is to study the results. • In this step, you will reflect on how the measured results compare with the predicted outcome. • Ask: Did we accomplish what we set out to do? • If so, continue on this path! • If not, identify what did not work and why. Ideas for PDSA Cycles: Study Stage
After completing your trial of the idea, reflect on how it compared with your aim statement. • Did you accomplish what you set out to do? • Did it result in an improvement as you expected? If so, continue on this path! • If not, as in the Oswego example, it is important to identify what didn’t work and set up a test of the revision in the next step of the PDSA cycle, the Act stage. Ideas for PDSA Cycles: Study Stage
You will have the most impact When you take the time to reflect on what workedムor didn’tand why. As you analyze your results, answer the following questions: • Was the change tested as planned? • Was the change successful in achieving the goal of the cycle? • Was the change an improvement? Ideas for PDSA Cycles: Study Stage