Download
1 / 60
1.25k likes | 3.42k Views
4. Disorganized Thinking. Confusion Assessment Method for the ICU (CAM-ICU). 1. Acute onset of mental status changes or a fluctuating course and 2. Inattention And. 3. Altered level of consciousness. or. = Delirium.

E N D
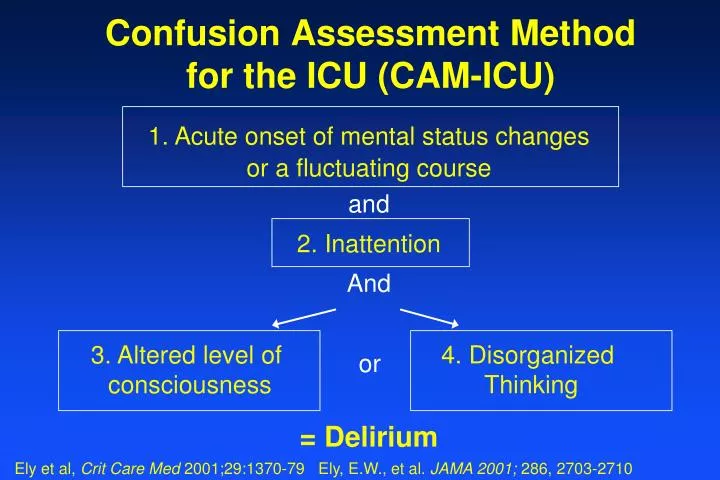
4. Disorganized Thinking Confusion Assessment Method for the ICU (CAM-ICU) 1. Acute onset of mental status changes or a fluctuating course and 2. Inattention And 3. Altered level of consciousness or = Delirium Ely et al, Crit Care Med 2001;29:1370-79 Ely, E.W., et al. JAMA 2001; 286, 2703-2710
Reliability and Validity of CAM-ICU • Compared CAM-ICU nurses’ and physicians’ rating to reference standard evaluation using DSM-IV expert psychiatric ratings • Validity ~95% • In 2 studies encompassing 150 patients and over 750 patient encounters • Inter-rater reliability ~ 0.92-0.96 Ely, Francis, Margolin et al, Crit Care Med 2001;29:1370-79 Ely, Inouye, Bernard et al, JAMA 2001;286:2703-2710
Adaption and Implementation • 15 languages and coming soon: Korean, Greek, Finnish, Thai • Harvard CAM-ICU flow sheet • pCAM-ICU (pediatrics) • CAM-ED (emergency department)
2002 Clinical Practice Guidelines* A joint Task Force of the Society of Critical Care Medicine (SCCM), American College Critical Care Medicine (ACCM), and the American Society of Health-System Pharmacists (ASHP) in alliance with the American College of Chest Physicians (ACCP). * Jacobi J, Fraser GL, Coursin DB, Riker R, Fontaine D, Wittbrodt ET, et al. Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med 2002; 30:119-141.
What the CAM-ICU measures...CAAM C– Change in Mental Status or Fluctuation A – Attention is Impaired A – Altered LOC or Arousal M – Muddled Thinking Both Required Only one Required
Screening/Presenting on Rounds 4 items in 10 seconds • Target RASS (team’s goal) • Actual RASS (arousal) • CAM-ICU (content) • Drugs (iatrogenesis imperfecta)
Teaching Point RASS & CAM-ICU Implementing sedation Scale (RASS) without delirium tool (CAM-ICU) … leaves only half of consciousness assessed (arousal not content) is clinically unsatisfying hurts compliance
+4 Combative +3 Very agitated +2 Agitated +1 Restless 0 Alert /calm -1 Drowsy eye contact >10 sec -2 Light sedation eye contact <10 sec -3 Moderate no eye contact -4 Deep physical stimulation required -5 Unarousable no response even with physical Step 1: Arousal Assessment (RASS) Verbal Stimulus Physical Stimulus Sessler CN, et al. AJRCCM 2002; 166:1338-1344. Ely et al, AJRCCM 2001;163:A954
Feature 1: Alteration/Fluctuation in Mental Status Is the pt different than his/her baseline mental status? OR Has the patient had any fluctuation in mental status in the past 24 hours (eg fluctuating RASS, GCS, previous delirium assessments, etc) Present: If either question is YES.
Feature 1: Alteration/Fluctuation in Mental Status Common Questions: • What if you do not know the patient’s baseline? • Assume normal unless you have red flags that make you suspicious • Red Flag: patient came from institution • What about dementia? • Ask family “What could she/he do prior to this illness?”
Feature 2: Inattention Screening for Attention– two options Letter “A” test Letters: S A V E A H A A R T (or numbers) Say 10 letters (or numbers) and instruct the patient to squeeze on the letter “A” (or on a certain number) Pictures Similar test with pictures (instructions are in picture packets)
Feature 2: Inattention 1. Attempt Letters first. 2. If pt is able to perform the Letter test you are sure of the results, you are done with Inattention test. 3. If pt is unable to perform the Letter test or you are unsure of the results, use the Pictures. If you perform both tests, use the Pictures result to determine if inattention is present. Inattention Present :If >2 errors
Teaching Point Inattention (Feature 2) This is THE cardinal feature and must be present to diagnose delirium. F2 is quick and simple. 95% of evaluations are done using only “hand squeezes” on correct letters or numbers. We need the picture method of screening for inattention in <5%, who are often very interesting patients.
Feature 2: Inattention Common Questions: • What if the patient only squeezes once and then falls back to “sleep”? or What if the patient is too hyperactive/combative to participate in squeezing? • Remember what you are assessing—Attention • This patient is inattentive • If you have to explain the directions more than twice, start to be suspicious for inattention
Teaching Point Hand Squeezing In the absence of other specific neurological diagnoses, a patient who squeezes on all letters, squeezes on NO letters, or misses >2 letters/numbers/pictures is inattentive and F2 positive. With a RASS other than “0,” he/she is delirious from many possible causes (e.g.: sepsis, sedatives, CHF).
4. Disorganized Thinking Confusion Assessment Method for the ICU (CAM-ICU) 1. Acute onset of mental status changes or a fluctuating course and 2. Inattention and 3. Altered level of consciousness or = Delirium Ely et al, Crit Care Med 2001;29:1370-79 Ely, E.W., et al. JAMA 2001; 286, 2703-2710
If either Feature 1 or 2 are absent, Stop Overall CAM-ICU is Negative If Features 1 and 2 are present, Proceed to Feature 3 Remember-Tailor your exam!
Feature 3: Alt Level of Consciousness Any LOC other than Alert. Present:If the Actual RASS score is anything other than “0” (zero). You have already done this assessment. It was the first thing you did when you walked in the room!
Teaching Point UTA The term ‘Unable to Assess’ is only recorded when patients are in stupor/coma (RASS -4/-5).
Feature 4: Disorganized Thinking Yes/No Questions(Use either Set A or Set B) : Set A Set B 1. Will a stone float on water? 1. Will a leaf float on water? 2. Are there fish in the sea? 2. Are there elephants in the sea? 3. Does one pound weigh more than 3. Do two pounds weigh two pounds? more than one pound? 4. Can you use a hammer to pound a nail? 4. Can you use a hammer to cut wood? Note: Use whatever form of communication that works (nodding, hand squeezing, blinking, etc).
Feature 4: Disorganized Thinking Command Say to patient: “Hold up this many fingers” (Examiner holds two fingers in front of patient) “Now do the same thing with the other hand” (Not repeating the number of fingers). • Patient gets credit only if able to successfully complete the entire command
Feature 4: Disorganized Thinking Present: If there is >1 error for the combined questions + command. • Notes: • If pt is unable to move both arms, for the second part of the command ask patient “Add one more finger”. • If patient is unable to move arms at all (quadriplegic), then feature 4 is presentif patient misses more than 1 question.
4. Disorganized Thinking Confusion Assessment Method for the ICU (CAM-ICU) 1. Acute onset of mental status changes or a fluctuating course and 2. Inattention And 3. Altered level of consciousness or = Delirium Ely et al, Crit Care Med 2001;29:1370-79 Ely, E.W., et al. JAMA 2001; 286, 2703-2710
What to THINK of when CAM+ • Toxic Situations • CHF, shock, dehydration • Deliriogenic meds • New organ failure, e.g, liver, kidney • Hypoxemia; also, consider giving Haloperidol or other antipsychotics? • Infection/sepsis (nosocomial), Immobilization • Nonpharmacological interventions • Hearing aids, glasses, reorient, sleep protocols, music, noise control, ambulation • K+ or Electrolyte problems
Delirium in the ICUClinical Value of RASS/CAM Measurement • Stimulates thinking of Rx: • Delirium Recognition is a Burglar Alarm for us • Forces us to consider treatable causes earlier • Avoid knee-jerk treatment with benzodiazepines • Consider haloperidol or atypical antipsychotic
DDx and Contributing Factors to Delirium Drugs Eyes, Ears Low O2 States (MI,Stroke,PE) Infection Retention (Urine or Feces) Ictal Underhydration, Undernutrition Metabolic Subdural DELIRIUMS
ANTIPARKINSONCV DRUGSINSOMNIAMUSCLE Relax. CORTICOSTER. H2 BLOCKERSNSAIDS SEIZURE URIN INCONTANTIBIOTICS THEOPHLLYINENARCOTICS EMPTYING DRUGSGERO-PSYCH ENT Drugs that can cause an ACUTE CHANGE IN MS Flaherty JH. Clinics in Geriatric Medicine, 1998
84 year old man, Admitted for CHF. Day 3 he feels better (less short breath) Day 4 he suddenly becomes agitated, uncooperative, confused. His urine output is less than before. Diagnosis? ?* Blackburn & Dunn, Arch Int Med 1990
Cystocerebral Syndrome*(Urinary Retention) Symptoms: pain, agitated delirium, overflow incontinence, acute renal failure Blackburn & Dunn, Arch Int Med 1990
The Treatment of Delirium is the Identificationand Treatment of the Underlying Causes
Medication to control agitation may exacerbate and prolong the course of delirium
4. Disorganized Thinking Confusion Assessment Method for the ICU (CAM-ICU) 1. Acute onset of mental status changes or a fluctuating course and 2. Inattention and (NEW) 3. Altered level of consciousness or = Delirium Ely et al, Crit Care Med 2001;29:1370-79 Ely, E.W., et al. JAMA 2001; 286, 2703-2710
Case #1: Mr. Icy 45 y/o man, lawyer with no previous memory or attention problem Dx: DKA, Intubated In the past 24hrs the RASS scores have been -3 to +1. Step 1: Sedation Assessment Currently: Awake and moving around restless in bed, but not aggressive. RASS = +1 What do we do next?
Case #1: Mr. Icy Step 2: CAM-ICU - Feature 1: Is he at his MS baseline? Fluctuation? - Feature 2: Letters = 6/10 - Feature 3: RASS = +1 - Feature 4
Case #1: Mr. Icy Step 2: CAM-ICU - Feature 1: Is he at his MS baseline? Fluctuation? Other RASS Scores: -3 +1 - Feature 2: Letters = 6/10 - Feature 3: RASS = +1 - Feature 4 Is this patient delirious??
Case #2 Mrs. Dapple 75 y/o female Dx: Severe pneumonia requiring prolonged mechanical ventilation and difficulty weaning In past 24 hours: RASS scores -3 to -1 Step 1: Sedation Assessment Asleep, but awakens to voice; maintains eye contact for >10 seconds RASS = -1 What do we do next?
Case #2 Mrs. Dapple Step 2: CAM-ICU - Feature 1: Is she at her MS baseline? Fluctuation? - Feature 2: Letters = 9/10 - Feature 3 - Feature 4
Case #2 Mrs. Dapple Step 2: CAM-ICU - Feature 1: Is he at his MS baseline? Fluctuation? RASS Variance: 2 - Feature 2: Letters = 9/10 - Feature 3 - Feature 4 Is this patient delirious??
Rest of CAM-ICU done anyway… • Something is amiss with this patient’s thinking. Rest of CAM-ICU shows disorganized thinking (Feature 4 +) • So… • Fluctuation of MS (Feature 1 +) • NOT inattentive (Feature 2 -) • LOC is “other than alert” (RASS -1, Feature 3 +) • Disorganized thinking (Feature 4 +)
What do you call this? • Delusions • Need to determine if having hallucinations • Subsyndromal delirium • Hyperactive Delirium
Teaching Point Subsyndromal Delirium Patients may have some features without the full syndrome of delirium (e.g., F2 only or F1&4 only). This is a (subsyndromal) intermediate state between normal and delirium. Reassess with CAM-ICU frequently to determine the clinical course of his/her emerging brain dysfunction.
Case # 3 Miss Universe Miss Universe was successfully extubated from the Vent at 0800. All sedation and analgesia had been stopped earlier in the AM. Yesterday evening and last night she had periods of agitation with a documented RASS range of -1 to +3. Step 1: Sedation Assessment Pt alert and calm. RASS = 0 What do we do next?
Case #3: Miss Universe Step 2: CAM-ICU - Feature 1: Is she at her MS baseline? Fluctuation? - Feature 2: Letters = 7/10, but you aren’t sure Pictures = 6/10 - Feature 3: RASS = 0 - Feature 4
Case #3: Miss Universe Step 2: CAM-ICU - Feature 1: Is she at her MS baseline? Fluctuation? RASS Variance = 4 - Feature 2: Letters = 7/10, but you aren’t sure. Pictures = 6/10 - Feature 3: RASS = 0 - Feature 4 Do you need to do Feature 4??
Case #3: Miss Universe Step 2: CAM-ICU - Feature 1: Is she at her MS baseline? Fluctuation? - Feature 2: Letters = 7/10, but you aren’t sure. Pictures = 6/10 - Feature 3: RASS = 0 - Feature 4: Answered half the questions wrong Unable to perform 2-step command Total Score: 2/5