Download
1 / 9
130 likes | 1.15k Views
Varicose Eczema/ Ulcers. Aetiology – inflammation due to toxin release from hypertensive veins in lower leg, in turn due to gradual superficial/ deep venous valve incompetence. Prevalence – v v (>40yrs) 15%( ♂) 27.5%(♀); Ulcers 0.3%- 2% (by age 80). Varicose Eczema/ Ulcers.

E N D
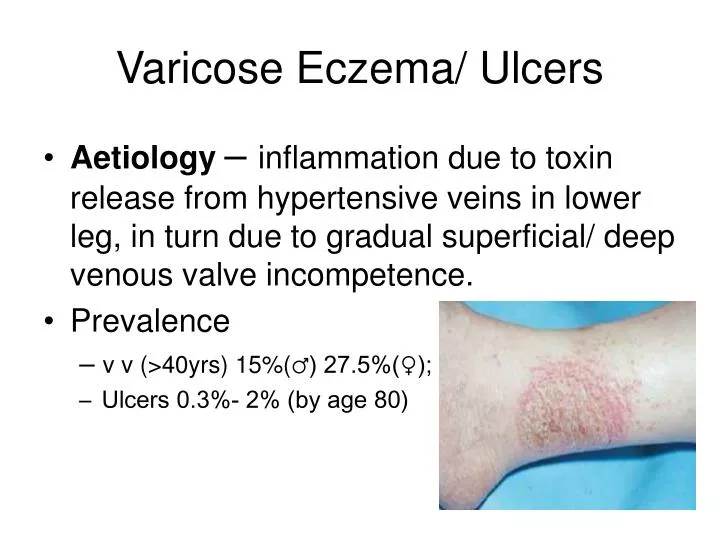
Varicose Eczema/ Ulcers • Aetiology– inflammation due to toxin release from hypertensive veins in lower leg, in turn due to gradual superficial/ deep venous valve incompetence. • Prevalence – v v (>40yrs) 15%(♂) 27.5%(♀); • Ulcers 0.3%- 2% (by age 80)
Varicose Eczema/ Ulcers • Contributing factors – age, 2+ pregnancies, obesity (female only), DVT, obstructed venous return, ?also smoking, prolonged standing and sitting. • Symptoms – itching, burning, aching especially at night-time, (odour with ulcers !).Pain should alert to arterial cause • Examination – erythema and excoriation medial calf above medial malleolus (LSV), post-inflammatory melanoderma. Oedema. Not usually painful even when shallow ulceration
Varicose Eczema/ Ulcers • Assessment. Examine lying and standing. Varicosities • Assess arterial supply (Doppler?) (anomalies in results due to oedema or arterial calcification)
Varicose Eczema/ Ulcers • Ulceration – team approach is vital. • Swab occasionally helpful if pseudomonas suspected (bright green exudate)
Varicose Eczema/ Ulcers • Beware of large ulcers and possible development of osteomyelitis
Varicose Eczema/ Ulcers Rx. – Compression = easily most important – provided arterial supply adequate (class 1-3, open/closed toe, knee or thigh length) • Emollients(?) • Systemic antibiotics for secondary infection (?)(Fluclox. +/- pen V/ amox. or erythromycin)
Varicose Eczema/ Ulcers • Ulcers • recent published meta-analysis • The type of dressing applied beneath compression was not shown to affect ulcer healing……applying hydrocolloid dressings beneath compression produced no benefit in terms of ulcer healing compared with applying simple low adherent dressings. No conclusive recommendations can be made as to which type of dressing is most cost effective. Decisions on which dressing to apply should be based on the local costs of dressings and the preferences of the practitioner or patient. (BMJ 2007;335:244) • Compression for all whose arterial supply is adequate (>0.7) • 4 layer bandaging
Varicose Eczema/ Ulcers • Can be difficult to apply compression hosiery (especially Classes 2 and 3) • Acti-glide can help
Varicose Eczema/ Ulcers • Elevation • Antibiotics if infected (rim of erythema and granulation at base with some exudate are normal ) • Be patient • Referral if enlarging or deepening