Download
1 / 25
290 likes | 828 Views
CORE NEEDLE BIOPSY IS HIGHLY ACCURATE IN DIAGNOSING BONE AND SOFT-TISSUE LESIONS. Piya Kiatisevi 1 , Torsten Nielsen 2 , Malcolm Hayes 2 , Peter L Munk 3 , Amy E LaFrance 4 , Paul W Clarkson 4 , Bassam A Masri 4

E N D
CORE NEEDLE BIOPSY IS HIGHLY ACCURATE IN DIAGNOSING BONE AND SOFT-TISSUE LESIONS Piya Kiatisevi1, Torsten Nielsen2, Malcolm Hayes2, Peter L Munk3, Amy E LaFrance4, Paul W Clarkson4, Bassam A Masri4 1Orthopaedic Oncology Lerdsin Hospital, Institute of Orthopaedics, Lerdsin Hospital, Bangkok, Thailand 2Department of Pathology and Laboratory Medicine, University of British Columbia, Vancouver, BC, Canada 3Department of Radiology, University of British Columbia, Vancouver, BC, Canada 4Department of Orthopaedics, University of British Columbia, Vancouver, BC, Canada Saturday, November 15, 2008
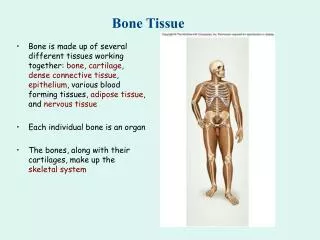
Background • Open biopsy is the historical gold standard for diagnosing bone and soft-tissue lesions • Highly accurate • 16% complication rate • 12% treatment altered • 1.2% unnecessary amputation Mankin et al., J Bone Joint Surg Am. 1996;78(5):656-663
Core Needle Biopsy (CNB) • Increasingly accepted for the diagnosis of bone and soft-tissue lesions • Reduced morbidity, time and cost • Fewer complications • Concerns remain regarding accuracy of CNB
Objectives • To assess and compare : • Core Needle Biopsy (CNB) • Open Biopsy (OB) • Fine Needle Aspiration (FNA) • Diagnostic rate • Accuracy for • Distinguishing benign vs. malignant • Histological diagnosis • Distinguishing low vs. high grade sarcoma
Materials and Methods • Prospectively collected database • 286 biopsies in 282 patients • 2004-2007 • 165 males, 117 females • Mean age 51 yrs (range 16-92 yrs) • Biopsy compared to final pathology • Included biopsies performed prior to referral but slides were re-reviewed by an experienced MSK pathologist
Our Practice • Patients are assessed in MSK surgical clinic • Site for CNB is marked with indelible marker • Image-guided biopsy performed by radiologist within pre-marked biopsy site • 10mm biopsy incision so site is identifiable for definitive resection
Our Practice • If core needle biopsy is non-diagnostic, then proceed with open biopsy • Biopsy track excised en bloc with tumour during definitive resection
Biopsy Types 229 CNB 286 biopsies 32 OB 25 FNA
Diagnostic Rate 92% 100%72%
Non-diagnostic Specimens CNB (18/229 = 8%) FNA (7/25 = 28%)
Accuracy for Distinguishing Benign vs. Malignant Accuracy89% 97%68%
Incorrect Diagnosis of Benign vs. Malignant • Benign (at biopsy) Malignant (final pathology) • CNB (n=229) • 6 Benign lipomatous tumour Well-differentiated liposarcoma (ST) • 1 Fracture healing Adenocarcinoma metastasis (B) • OB (n=32) • 1 Leiomyoma Leiomyosarcoma (ST) • FNA (n=25) • 1 Mature fat Well-differentiated liposarcoma (ST)
Incorrect Diagnosis of Benign vs. Malignant • Malignant (at biopsy) Benign (final pathology) • CNB (n=229) • 1 Lymphoma of ilium Osteomyelitis (B) • OB (n=32) • 0 • FNA (n=25) • 0
Accuracy for Histological Subtype Accuracy 70% 81% 40%
Accuracy for Distinguishing Low vs. High Grade Sarcoma Accuracy90% 96% 72%
Incorrect Diagnosis of Low vs. High Grade Sarcoma • Low grade (at biopsy) High grade (final pathology) • CNB (n=92) • 3 • OB (n=24) • 0 • FNA (n=10) • 2 • High grade (at biopsy) Low grade (final pathology) • None 1 Osteosarcoma (B) 1 Liposarcoma (ST) 1 Ossifying fibromyxoid tumour (ST) 1 De-diff. Chondrosarcoma (B) 1 Myofibroblastic sarcoma (ST)
Discussion • Perform CNB with care on fatty lesions
Conclusion • Core needle biopsy is accurate for determining: • Benign vs. malignant • Histological subtype • Low vs. high grade for sarcoma • Advantages of core needle biopsy • Fewer complications • Reduced cost of treatment • High diagnostic accuracy
Recommendations • CNB be used routinely for diagnosis, whenever possible • Open biopsy reserved for use when CNB is non-diagnostic • Given its high inaccuracy, FNA is not indicated for diagnosing musculoskeletal lesions in the extremities
Orthopaedic Oncology Lerdsin Hospital, Bangkok, Thailand Thank you The University of British Columbia, Vancouver, BC, Canada