Download
1 / 86
880 likes | 1.87k Views
Katie Dolbec, MD. Frostbite and Dermal Cold Injury. The Case. A 48-year-old gentleman is brought to the ED by EMS.

E N D
Katie Dolbec, MD Frostbite and Dermal Cold Injury
The Case • A 48-year-old gentleman is brought to the ED by EMS. • His roommate found him staggering back into his house after being outside. The patient got into a fight with his roommate and overdosed on Ambien - possibly up to sixty 5-mg tablets. • The patient went outside for an unclear period of time. He fell while he was outside, striking his face on a woodpile. He apparently lost consciousness and then was outside in the bitter cold with temperatures at 0 degrees. • His core temperature on arrival is 32oC by Foley catheter. He has evidence of significant frostbite of both hands with limited range of motion of his fingers and toes; his hands are frozen, discolored red and white and without capillary refill. He also has evidence of superficial frostbite of his knees and his left elbow. • His tetanus is up-to-date. • He does not smoke cigarettes.
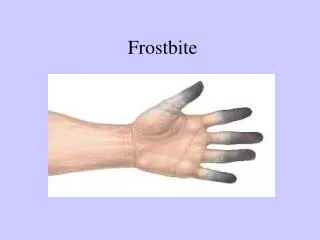
Frostbite Definition • Freezing injury of tissue • Ice crystal formation in superficial or deep structures
Epidemiology – Risk Factors • Alcohol consumption (46%) • Motor vehicle problems (19%) • Psychiatric illness (17%) • Vehicular failure (15%) • Drug misuse (4%) • Homelessness • Military • Recreational and athletic participants • Improper clothing • History of previous cold injury • Fatigue • Dehydration • Wound infection • Atherosclerosis • Diabetes • Smoking • High Altitude, Hypoxia • African American race • Being raised in the south • Excessive sweating • (Elderly, Young children) • Age 30-49 • Male Sex (10:1) Psych/Behavioral (and car troubles) Vascular Genetic/Inherent
Epidemiology • Incidence unknown • Common anatomic locations • Feet • Hands • Ears • Nose • Cheeks • Penis
Hershkowitz M. Penile Frostbite, an Unforseen Hazard of Jogging. New England Journal of Medicine. Jan 20, 1977.
Travis S, Roberts D. Arctic Willy. BMJ, Vol. 299, 23-30 December 1989.
Epidemiology • Population at risk for co-existing conditions • Consider & manage: • Hypothermia • Trauma
Pathophysiology • Frostbite occurs when tissue heat loss exceeds the ability of local tissue perfusion to prevent freezing of tissues • 4 Overlapping phases of tissue cooling: • Prefreeze phase • Freeze-thaw phase • Vascular stasis phase • Late ischemic phase
Pathophysiology – Prefreeze Phase • Tissue cooling <10oC • Sensation is lost at 10oC • Vasoconstriction • Hunting reflex (cold-induced vasodilation) • Episodes of transient vasodilation every 7-10 min • Disappears with prolonged exposure to cold • Ischemia • No ice crystal formation
Pathophysiology – Freeze-Thaw Phase • Temperatures between -6oC and -15oC • Ice crystals form intracellularly (rapid freeze) and/or extracellularly (slow freeze) • Cellular damage • Thawing initiates reperfusion injury and inflammatory response
Pathophysiology – Vascular Stasis Phase • Vessels alternate between constriction and dilation • Blood leaks from vessels or coagulates within them
Pathophysiology – Late Ischemic Phase • Ongoing reperfusion injury • Inflammatory cascade • Intermittent vasoconstriction • Microvascular emboli/macrovascular thrombi • Progressive tissue ischemia and infarction
Pathophysiology • Mechanisms of Tissue Damage: • Cellular injury • Tissue ischemia • Inflammatory mediator release
Pathophysiology – Cellular Injury • Extracellular and intracellular ice crystal formation • 1) Extracellular ice increases extracellular oncotic pressure • Water moves out of cells • Cellular electrolyte, pH shifts • Cellular dehydration • Protein and lipid derangement • Cell membrane lysis • 2) Intracellular ice causes disruption of cell membranes • With thawing, tissue edema ensues ***Cellular necrosis***
Pathophysiology – Tissue Ischemia • Local vasoconstriction • Increased blood viscosity • Microvascular damage • Endothelial disruption • Transcapillary plasma loss • Edema • Further limitation of blood flow • Endothelial damage microthrombi formation • Freeze-thaw-refreeze increases severity of thrombosis and ischemia
Immediately after thawing blood flows freely • Five-ten minutes post-thaw blood begins to sludge • Clot • Ischemia • Necrosis
Frostbitten skin from rabbit ear transplanted autogenously to normal ear • Normal skin transplanted to frozen area • Frostbitten skin survived on normal tissue bed • Normal skin necrosed on frostbitten bed Weatherly-White RCA, Sjostrom B, Paton BC. Experimental Studies in Cold Injury. Journal of Surgical Research; 1964 (Jan): Vol. IV, No. 1.
Pathophysiology - Inflammatory Mediator Release • Secondary effect of pro-inflammatory cytokine release • Thromboxane A2 • Prostaglandin F2-alpha • Bradykinin • Histamine • Exacerbates cellular damage • Causes further ischemia • Vasoconstriction • Platelet aggregation • Blood vessel thrombosis Found in frostbite blister fluid
Tissue frozen and thawed twice sustained greater injury • Double 3-min freezes caused more damage than a continuous 6-minute freeze Hardenbergh E, Ramsbottom R. Experimental Frostbite: The Effect of “Double Freeze” on Tissue Survival in the Mouse Foot. Cryobiology, Vol. 5, No. 5, 1969
Reamy BV.Frostbite: Review and Current Concepts. Journal of American Board of Family Practice, Jan. – Feb. 1998, Vol. 11, No. 1
Frostnip • Superficial non-freezing cold injury • Tends to occur on exposed skin • Ears, cheeks, nose • Intense vasoconstriction • Ice crystals (frost) form on skin surface • Indicates favorable conditions for frost bite ***DOES NOT EQUAL FROSTBITE*** ***RESULTS IN NO TISSUE LOSS*** ***NO LONG-TERM SEQUELAE***
First-degree Frostbite • White or yellow firm, slightly raised plaque • Numbness • No gross tissue infarction • Slight epidermal sloughing • Mild edema
Second-degree Frostbite • Superficial skin vesiculation • Clear or milky fluid in blisters • Surrounding erythema and edema
Third-degree Frostbite • Deeper, hemorrhagic blisters • Injury has extended into reticular dermis and dermal vascular plexus
Fourth-degree Frostbite • Extends through the dermis • Involves subcutaneous tissues • Necrosis extending into muscle and to bone
Two-Tiered Classification System • Better in the field • More of a clinical diagnosis • Superficial frostbite • Deep frostbite
Superficial Frostbite • No or minimal anticipated tissue loss • Corresponds with 1st- and 2nd-degree injury • Treat conservatively • Favorable prognostic factors: • Retained sensation • Normal skin color • Clear blisters • Blisters only in distal phalanges
Deep Frostbite • Deeper injury and anticipated tissue loss • Corresponds with 3rd- and 4th-degree injury • Requires aggressive management • Poor prognostic features: • Nonblanching cyanosis • Absent Doppler pulses • Firm skin • Dark, fluid-filled (hemorrhagic) blisters • OR • Little or no blister formation (even worse)
Prevention • Pathophysiology told us that tissue perfusion has to exceed heat loss… • Maintain peripheral perfusion • Blood flow = heat • Allow heat to get to tissues • Protection from the cold • Prevent heat loss
Maintaining Peripheral Perfusion • Maintain core temperature • Hydration • Adequate nutrition • Minimize effects of known diseases or perfusion-limiting drugs (including smoking) • Cover skin – prevent vasoconstriction • Prevents restriction to blood flow • Prevent hypoxemia with supplemental O2 if needed • Exercise* • Raises core temperature and causes vasodilation • *Leads to exhaustion
Protection from the Cold • Protect skin • Emollients DO NOT protect skin & actually increase risk • Avoid perspiration or wet extremities • Increase insulation & skin protection – layers • Avoid alcohol/drugs/hypoxemia • Allows you to respond behaviorally to changing conditions • Use chemical hand and foot warmers, electric foot warmers • Perform “cold checks” • Recognize frostnip & superficial frostbite early • Minimize duration of cold exposure • Avoid environmental conditions favorable for frostbite
Weather Conditions & Frostbite • Ambient air temperature • Frost nip doesn’t generally happen until skin temperature is below -6 degrees C • Skin rarely freezes above -15 to -10 degrees C (+5 to +14 F) • Skin will readily supercool • Cold-induced vasodilation occurs; skin temperature levels off • Rate of air movement (wind speed) • Duration > temperature of exposure • Skin surface moisture • Contact with cold objects Wilson O, Goldman RF. Role of air temperature and wind in the time necessary for a finger to freeze. Journal of Applied Physiology. Nov 1970.
Emollients • Traditionally used by Finnish reindeer herders to prevent frostbite • Large prospective epidemiological study • 913 frostbite cases, 2,478 uninjured controls • Use of protective ointments associated with increased risk of frostbite on face (OR 3.3), nose (OR 5.6) and ears (OR 4.5) • Prospective experimental study • 24 young, healthy male subjects (med students) • Placed in a climatic chamber • 4 emolients tested on ½ the face • Thermistor and infra-red scanner temperatures • Emolients do not delay cooling of facial skin • Skin cooler on treated half in the majority of tests Lehmuskallio E. Rintamaki H. Anttonen H. Thermal Effects of Emollients on Facial Skin in the Cold. Acta Derm Venereol. 2000. Lehmuskallio E. Emollients in the Prevention of Frostbite. International Journal of Circumpolar Health, 2000; 59: 122-130.
Management • In the field: • If re-freezing is likely • If thaw is maintainable • Hospital setting: • Early treatment • Long-term treatment options
Field Management of Frostbite • General Guidelines: • Treat concomitant hypothermia • Before treating frostbite if moderate-severe • Maintain hydration • Administer ibuprofen (600mg BID-QID) • Blocks arachidonic pathway – decreased PGF2 and TxA2 • Protect the frozen part • Do not rub • Do not actively thaw if re-freezing is possible • Caveat: consider thawing if hospital is in distant future • Avoid re-freezing a thawed part • Do not prevent thawing if it is going to happen spontaneously
Field Management of Frostbite • If re-freezing is possible or inevitable: • Apply clean, bulky dressings to the frozen part and between toes and fingers • Avoid ambulation and pressure on frozen extremity – minimize additional trauma • If use is unavoidable: • Pad well • Splint • Immobilize as much as possible
Field Management of Frostbite • If thaw can be maintained: • Rapidly rewarm • Warm water immersion bath (37-39 degrees C) • Dry by blotting (avoid rubbing) • Antiseptic solution • Theoretical benefits, but no evidence • Pain control • NSAIDs • Opiates
Field Management of Frostbite • If thaw can be maintained, continued: • Do not debride blisters • Apply topical aloe vera • Reduces prostaglandin and thromboxane formation • Only beneficial for superficial injuries • Bulky, clean dressings wrapped loosely (swelling) • Avoid ambulation if possible • Elevate the injured extremity • Provide supplemental oxygen if hypoxia is present or at high altitude (>4000m)
Field Management of Frostbite McIntosh SE. Hamonko M, et al. Wilderness Medical Society Guidelines for the Prevention and Treatment of Frostbite. Wilderness and Environmental Medicine, 2011(22):156-166.
Hospital Management of Frostbite • Impossible to ascertain prognosis immediately after thawing • Immediate therapeutic options: • Treatment of hypothermia, trauma • Rapid rewarming of frozen tissues • Water bath (37-39oC) • Hydration • Topical aloe vera
Hospital Management of Frostbite • Immediate therapeutic options, continued: • Debridement of blisters • Selectively needle aspirate clear blisters • Leave hemorrhagic blisters intact • Systemic antibiotics • Cover Staph aureus and Pseudomonas aeruginosa • No need for universal antibiotic coverage • Tetanus prophylaxis • Low molecular weight dextran
Low Molecular Weight Dextran • Polysaccharide plasma expander • Proposed mechanism of action in frostbite: • Decreases blood viscosity • Inhibits intravascular cellular aggregation and improves small vessel perfusion
Low Molecular Weight Dextran • Pro: • Mundth ED, et al. 1964. • Improves tissue survival if given PRIOR TO freezing • May improve tissue survival if given one hour after rewarming and BID x5 days • Webster DB, et al. 1965. • Animals treated with LMWD before and after freezing injury had less necrosis than controls • Con: • Penn I, et al. 1964. • LMWD therapy associated with increased edema • Increased compression of blood vessels & interference of blood flow through injured area • No significant reduction in the amount of tissue loss
Low Molecular Weight Dextran • Take-home: • LMWD is worth considering if you can get it into the patient before the injury or within a couple of hours of presentation • …but it should not be given immediately • Most recent research is in the 1960s • We probably have better options
Hospital Management of Frostbite • Imaging options • Technetium 99 (Tc-99) triple phase scanning • Magnetic resonance angiography • Angiography • These help determine extent of tissue ischemia
Hospital Management of Frostbite • Thrombolytic therapy • Angiography, Technetium-99, or MR-A • IV or IA tPA within 24 hours of thawing may salvage some or all tissue at risk • Should only be considered in deep frostbite with potential for significant morbidity (proximal to interphalangeal joints) • Consider risks and contraindications • Heparin therapy as adjuvent to tPA (+/- warfarin)
Prospective study • 19 patients over 14 years • 6 intra-arterial tPA • 0.075 mg/kg/hr x6 hrs • 13 intra-venous tPA • 0.15 mg/kg bolus, then 0.15 mg/kg/hr x 6 hrs • No complications with IV tPA; 2 IA patients with bleeding • 16/19 patients responded to tPA • Equal efficacy with IV and IA • IV tPA is safe & reduced predicted digit amputations Twomey JA, Peltier GL, Zera RT. An Open-Label Study to Evaluate the Safety and Efficacy of Tissue Plasminogen Activator in Treatment of Severe Frostbite. The Journal of Trauma 2005 (Dec); Volume 59, Number 6, pp. 1350-1355.