Download
1 / 18
180 likes | 392 Views
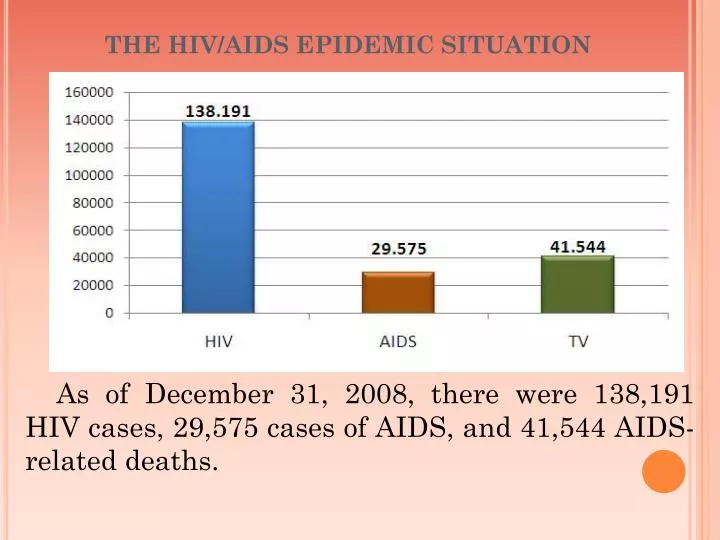
THE HIV/AIDS EPIDEMIC SITUATION. As of December 31, 2008, there were 138,191 HIV cases, 29,575 cases of AIDS, and 41,544 AIDS-related deaths. VIETNAM HIV/AIDS SITUATION AND POLICY ON MOBILITY AND HIV VULNERABILITY REDUCTION. THE HIV/AIDS EPIDEMIC SITUATION.

E N D
THE HIV/AIDS EPIDEMIC SITUATION As of December 31, 2008, there were 138,191 HIV cases, 29,575 cases of AIDS, and 41,544 AIDS-related deaths.
VIETNAM HIV/AIDS SITUATIONAND POLICY ON MOBILITY AND HIV VULNERABILITY REDUCTION
THE HIV/AIDS EPIDEMIC SITUATION • In 2008, 20,260 people were detected as having been infected with HIV/AIDS nationwide, 7,452 patients of AIDS, and 3,526 AIDS-related deaths • In comparison with 2007, there is a decrease of detected HIV infections (26.6%), AIDS patients (14.35%) and AIDS-related deaths (18.75%) in 2008.
PERCENTAGE OF WARDS/COMMUNES, DISTRICTS, PROVINCES/CITIES HAVING PLWA As of December 31, 2008, HIV-infections have been reported nationwide in 70.51% of wards/communes, 97.53% of districts and 63/63 provinces/ cities. In comparison with 2007, there are 03 more districts and 337 wards/communes having people living with HIV.
PROPORTIONS OF HIV INFECTIONS IN GENDERS According to detection surveillance data, the number of HIV infected men were four times higher than that of HIV infected women; men accounted for 82,04% and women accounted for 17,96%
HIGH HIV PREVALENCE AMONG IDUS - 20.27% of injecting drug users were HIV-infected in 2008. HIV prevalence is very high among IDUs in some provinces/cities Nguồn: Kết quả Giám sát trọng điểm 1994 - 2008 Provinces/cities with high HIV prevalence: - Ho Chi Minh city 50%, - Thai Nguyen 38.59%, - Can Tho46.07%, - QuangNinh33.25%. - Dien Bien 40.26%,
HIGH HIV PREVALENCE AMONG FWS 3.12% of female sex workers were HIV-infected in 2008 Exceptionally high in some provinces/cities: - Dien Bien 14.96%, - Ha Noi12.25%, - HaiPhong 10.75%.
LOW HIV INFECTION RATE AMONG PRENATAL WOMEN The HIV infection rate among prenatal women fluctuated from 0.02% in 1994 to 0.37%. Then, this rate slightly declined in recently.
LOW HIV INFECTION RATE AMONG MILITARY RECRUIT The HIV infection rate among young people taking medical examination in military recruit increase from 0% in 1994 to 0.95% in 2000. Then, this rate gradually decrease 0.12% in 2006. According sentinel surveillance data, the HIV infection rate among this group increase 0.27% in 2008.
CONCLUSION 1. Vietnam’s HIV transmission pattern is still in a concentrated phase, with the high sero-prevalence among injecting drug users (IDUs) and female sex workers (FSWs) but low in other populations.
2. Although the speed of a widespread of HIV/AIDS epidemic has been reduced in comparison with the previous years, basically, it has not been controlled yet. 3. Regardless of a declined trend of the epidemic, there will be a potential outbreak of the epidemic unless effective preventive measures are effectively implemented.
VIET NAM International, regional , National commitments, coordination and planning ON MOBILITY AND HIV VULNERABILITY REDUCTION
international or regional instruments relating to migrants, mobile populations and HIV vulnerability reduction Viet Nam endorsed the United Nations General Assembly Special Session (UNGASS) Declaration of Commitment on HIV/AIDS in June 2001 Viet Nam signed (MOU) for Joint Action to Reduce HIV Vulnerability to Population Movement between the Cambodia, China, Lao ; Myanmar, (2004-2009) in September 2004 Viet Nam signed the ASEAN Commitments on HIV and AIDS, and the ASEAN Declaration on the Protection and Promotion of the Rights of Migrants Workers, on 13 January 2007, in Cebu, Philippines Viet Nam endorsed the Regional Strategy on Mobility and HIV Vulnerability Reduction in South East Asia and Southern China 2006-2008 on 29th January 2007 Viet Nam was involved in the development of the APEC HIV/AIDS Workplace Guidelines (in close consultation with the International Labour Organization and based on the ILO ‘Code of Practice on HIV/AIDS and the World of Work’). The APEC Guidelines were endorsed by the APEC Economic Leaders in 2007
country reviewed and, where necessary, amended its multisectoral strategy/action framework to include migrants and mobile populations in March 2004 , The National Strategy on the Prevention and Control of HIV/AIDS in Viet Nam until 2010 with Vision to 2020 was adopted. The Strategy acknowledges the complexity of migration and mobility, and the underlying HIV vulnerability among key population groups The Law on HIV/AIDS Prevention and Control was adopted by the National Assembly on 29th June 2006. The Law includes a definition of mobile populations and a reference to HIV prevention and control among mobile populations. The Prime Minister’s January 2007 Decision on ‘Mechanism for Collaboration on Cross-border HIV/AIDS Prevention and Control’ provides the principles, It also describes the responsibilities of ministries, sectors, and People’s Committees at all levels of Viet Nam for collaboration with countries sharing borders Among nine National Programmes of Action in the National HIV Strategy, three include migrants and mobile populations as one of the target populations. The Viet Nam Administration of AIDS Control (VAAC) led a team consisting of various sectors, representatives of PLWHA, and migrants and mobile populations to develop guidelines on HIV prevention among migrants and mobile populations in Viet Nam. The guidelines were approved in August 2008 by the Director of VAAC. [
Government informed all affected Ministries and Departments (including agriculture, construction, finance, health, home affairs, labour, public works, public security, transport, and women’s affairs) of these agreements These agreements have been disseminated to all related ministries and branches through official channels. Dissemination of this information to various departments and the administrative, implementation level of government is responsibility of the related ministry. The Ministry of Labour, War Invalid and Social Affairs (MOLISA) is mainly responsible for overseas migrant workers. The Ministry of Agriculture and Rural Development (MARD) is responsible for overseeing the relocation of populations affected by large infrastructure projects and other rural resettlement programmes.
country have a mobility technical working group on HIV and AIDS (MTWG) to provide information sharing, coordination, and technical assistance Since 2005, the Department of Social Evils Prevention has convened the Mobility Technical Working Group (in Viet Nam it is titled the ‘Multi-sectoral Team on HIV and Mobility’) to bring together representatives from a variety of ministries and offices to address HIV and mobility. This team includes various offices of MOLISA, the Ministry of Health, the Ministry of Construction, the Ministry of Justice, the Ministry of Transportation, the Department for Social Affairs (Office of the National Assembly), the Institute of Sociology, the Viet Nam Association of Sociology, the Institute of Social Development Studies, the Viet Nam Chamber of Commerce and Investment, the Women’s Union, and representatives of people living with HIV, migrants and mobile populations.
Challenge and the way to forward The Law on HIV/AIDS Prevention and Control states that mobile populations are prioritized for access to information, education and communication on HIV prevention and control, and defines roles and responsibilities of concerned agencies in IEC. However there needs to be a mechanism in place to ensure IEC and BCC programmes are carried out properly and regularly. Appropriate state funding for such programmes should also be made available. The government should require an HIV impact assessment in the feasibility-study phase of major construction and infrastructure development projects and that integration of HIV prevention programmes should be required as a precondition for these projects. There is a need for guidance (or example, an Inter-Ministerial Circular) on the implementation of Article 19 of the Government’s Decree No.108/2007 ‘Integration of HIV/AIDS prevention activities into socio-economic development programmes’ with a focus on mobile populations. In each infrastructure construction project, health care and HIV prevention should be included as a required item with a separate budget line. The health sector should consider the issuance of a new kind of ‘mobile’ health insurance for mobile populations so that they can get access to health care and treatment wherever they are. The business sector should proactively engage in HIV prevention programmes for migrants and mobile populations. At the same time, the government should consider developing a policy to reduce applicable taxation, as an encouragement, for those enterprises that carry out HIV prevention activities for their employees with funding from their own income source.
Challenge and the way to forward The Mobility Technical Working Group was established and functioned well during the time the MTWG was facilitated by CSEARHAP. Coordination and cooperation between agencies participating in the MTWG have improved considerably and a lot of activities have been jointly conducted. In order to continue the momentum, the MTWG should be continued. The government should take the lead and consider turning the MTWG into an official functional technical working group on HIV and mobility in Viet Nam. A post-arrival, and returnee programme with information on migration, culture, health, and HIV, as well as laws and resources of host communities should be initiated and integrated into the current Pre-departure Training Programme. Such a programme could be integrated with or implemented alongside other existing HIV-related prevention programmes at sectoral and local levels as well. Although policies to promote comprehensive HIV and AIDS care and support, as well as improved access to HIV treatment for the populations are in place, there is still a need to consider a more specific policy for migrants and mobile populations in particular, taking into account their specific mobility and vulnerability to HIV. Cross-border collaboration on HIV prevention with neighbouring countries, particularly for undocumented migrants and mobile populations, should be enhanced by implementing the Decision on Mechanisms for Collaboration on Cross-border HIV/AIDS Prevention and Control.