Download
1 / 27
280 likes | 588 Views
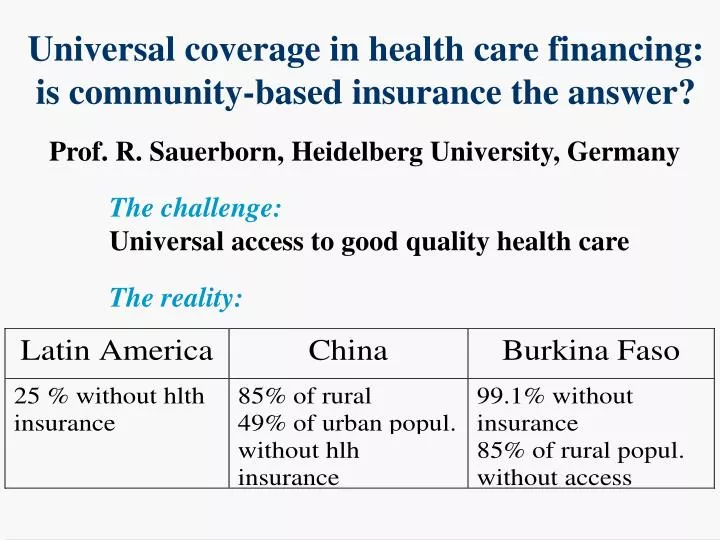
Universal coverage in health care financing: is community-based insurance the answer?. Prof. R. Sauerborn, Heidelberg University, Germany. The challenge: Universal access to good quality health care. The reality:. Main groups not covered by insurance.

E N D
Universal coverage in health care financing: is community-based insurance the answer? Prof. R. Sauerborn, Heidelberg University, Germany The challenge: Universal access to good quality health care The reality:
Share of informal sector in non-agricultural employment, Latin America
Per capita health expenditure by source - rural Burkina Faso 1996 F CFA
Overview of financing mechanism • fee for service - most developing countries • taxes - UK • saving funds - Singapore • private insurance - US • HMO - US • social insurance - German and Latin American model • community-based insurance - experiments from Africa, Latin America, Asia
Target groups forsocial and voluntary insurance -Vietnam, 1999 Total population 78 m Informal sector Civil servants, Dependents fomal sector self-employed in need of incl. retirees rural workers coverage 8m 38 m 32 m Social insurance Voluntary User fees Government Donor aid insurance subsidies ca 2 m 8 m 4m 34 m ca 30 m 41 % 10 % 5 % 44 % Jowett and Thompson, 1999
Spreading financial risks protects the livelihood of poor households
Definition:Community-based health insurance: Applying the principles of insurance to the social context of communities, guided by their preferences and based on their structures and arrangements.
Approach to create CBI (I) • Identify the excluded
Example: The main groups not covered by insurance in Chinese Cities: • primary dependents of people covered under the government health insurance (gongfei) and workers’ insurance (laobao) • people employed by private companies and joint ventures • self-employed (getihu) • rural to urban migrants
Approach to create CBI (II) • Identify the excluded • Understand the informal sector organizations and the existing risk-sharing arrangements
Types of community risk sharing organizations- Nouna district, rural Burkina Faso- name function # organizations # participating individuals 150 in district Tontines Traditional saving groups 2,388 (rotative savings) (Nouna has 17) Pre-cooperatives Saving, food aide, social 43 2,000 activities, transport, rotative Cooperatives farming and harvesting, 1 47 house and well construction Associations tree planting, road construction, 13 2,800 crafts, environmental hygiene, health (1) 7,235 207 (= 12.1% of population) Source: Sauerborn et al., 1998
Approach to create CBI (III) • Identify the excluded • Understand the informal sector organizations and the existing risk-sharing arrangements • Study community preferences for benefit package content • Assess willingness-to-pay for such packages
Comparative research: Willingness-to-pay for community-based health insurance
Approach to create CBI (IV) • Assess population-based health care needs • Establish unit costs of service provision • Calculate premium
Germany 1883-2000: gradual increase in social insurance coverage Year 1885 1895 1910 1914 1925 1934 1950 1955 1960 1965 1968 1976 1980 1985 1990 1995 100 Private health insurance Statutory health insurance 90 80 70 Coverage in % of total population 60 50 40 30 20 10 0
Germany 1883-2000: consolidation of sickness funds 120000 25000 number of statutory sickness funds average number of insured per fund 100000 20000 80000 Number of statutory sickness funds 15000 60000 Average number of insured per fund 10000 40000 5000 20000 0 0 1885 1895 1905 1915 1925 1935 1945 1955 1965 1975 1985 1995 Year
From community-based health insurance to universal coverage Mechanisms: • public regulation • amalgamation • re-insurance • risk equalisation scheme
Closing the circle • Global health problems- global solutions • Example: Health sector crisis - financing of high quality care through insurance • Evidence from different places and times may be instructive
Health care crisis Cooperation Isolation