Download
1 / 14
140 likes | 283 Views
Creating an Integrated Framework for Reducing Disparities in Health Care Quality. Francis D. Chesley, Jr., MD Director Office of Extramural Research, Education and Priority Populations AHRQ Annual Conference September 28, 2010. The Change/Evolution of AHRQ.

E N D
Creating an Integrated Framework for Reducing Disparities in Health Care Quality Francis D. Chesley, Jr., MD Director Office of Extramural Research, Education and Priority Populations AHRQ Annual Conference September 28, 2010
The Change/Evolution of AHRQ President’s FY 2011 AHRQ budget proposal: $611 million AHRQ begins sponsorship of U.S. Preventive Services Task Force activities FY 2003 Budget: $318.7 million FY 2010 Budget: $397 million FY 1990 Budget: $97 million FY 1995 Budget: $154 million 1989 1995 1998 2000 2005 2010 Agency for Health Care Policy and Research (AHCPR) is established AHCPR becomes the Agency for Healthcare Research and Quality (AHRQ) “Near-death experience” Effective Health Care (EHC) Program created Recovery Act Funding in 2009: $300 million to AHRQ EHC Program launched, includes dissemination and application function by the Eisenberg Center
Setting the Context • The Healthcare Research and Quality Act of 1999 directed AHRQ to conduct and support research with respect to the delivery of health care for Priority Populations • AHRQ published its Priority Population Inclusion Policy in February 2003 • Established an AHRQ functional unit to assist in carrying out policy requirements
AHRQ Priority Populations • Inner city and rural areas (including frontier areas) • Low income groups • Racial and ethnic minority groups • Women and children • The elderly • Individuals with special health care needs, including individuals with disabilities and those who need chronic care or end-of-life health care
The Policy • Provides one of the cornerstones for studying and eliminating health care disparities • Intended to ensure inclusion in AHRQ’s overall portfolio of research • Intended to foster inclusion such that research designs explicitly allow for valid analyses – including subgroup analyses where relevant • Investigators should consider inclusion of one or more priority populations
The Policy (cont) • Encourages development of specific outreach plans to reach participant recruitment goals • Encourages subgroup analyses to provide specific research results relevant to one or more priority population • Requires explicit justification of exclusion, such as inappropriate with respect to the health of subjects or purpose of research
Inclusion in Real Time • Core Business • Knowledge Creation • Synthesis & Dissemination • Implementation & Use • Measurement • Data • Training & Research Infrastructure • Research Portfolios
AHRQ Portfolios • Value • Goal: Support the development of health care activities that help reduce unnecessary waste while improving quality • Innovations/Emerging Issues • Goal: Identify and support ideas and projects that have the potential for highly innovative solutions to health care challenges
AHRQ Priorities Patient Safety • Health IT • Patient SafetyOrganizations • New PatientSafety Grants Effective HealthCare Program AmbulatoryPatient Safety • Comparative Effectiveness Reviews • Comparative Effectiveness Research • Clear Findings for Multiple Audiences • Safety & Quality Measures,Drug Management andPatient-Centered Care • Patient Safety ImprovementCorps Other Research & Dissemination Activities Medical ExpenditurePanel Surveys • Visit-Level Information on Medical Expenditures • Annual Quality & Disparities Reports • Quality & Cost-Effectiveness, e.g.Prevention and PharmaceuticalOutcomes • U.S. Preventive ServicesTask Force • MRSA/HAIs
Lessons Learned Common application statement – priority populations will be included in our study to extent that they exist in our study population How do I comply when I am using secondary data and subgroup numbers are small? But also, AHRQ should be explicit about specific priorities for priority populations research in each Funding Opportunity Announcements Are there “points” in peer review and funding decision making?
Lessons Learned • Policy of encouragement difficult to understand and implement • True inclusion and subgroup analyses require resources • Specific role for peer review • Factoring inclusion as a component of funding decisionmaking is not easy • We need a framework!
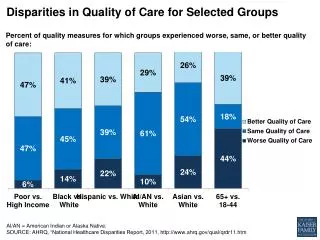
Why Is This Important? • Health care disparities persist and in many cases are worsening • Ongoing and enhanced focus & activities within the DHHS • Recognized importance of quality improvement must include strategies for eliminating disparities • The ACA requires establishment of offices of minority health in HHS and focus on eliminating health disparities • The ACA calls for National Quality and Prevention Strategies – each includes eliminating disparities as a core principle
ACA Provisions Related to AHRQ • Community Health Team to Support Patient-Centered Model Home • Medication Management Services • Improving the Emergency Care System • Shared Decision Making • Collecting Data on Health Disparities • Health Care Workforce • Primary Care Extension Service • Medical Liability* *Only item on the list with an appropriation. All other items authorized.
Thank You AHRQ Mission To improve the quality, safety, efficiency, and effectiveness of health care for all Americans AHRQ Vision As a result of AHRQ’s efforts, American health care will provide services of the highest quality, with the best possible outcomes, at the lowest cost http://www.ahrq.gov